3.10 Atrial Fibrillation
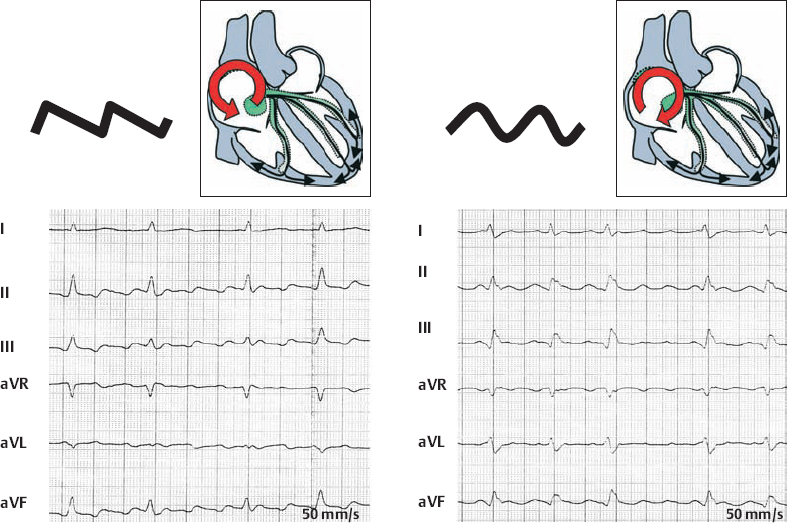
Comparison of Isthmus-Dependent “Typical” Atrial Flutter (Counter-Clockwise vs. Clockwise)
Atrial Fibrillation—In General
Atrial Fibrillation—Treatment, Rhythm Control vs. Rate Control, Prevention of Thrombembolism
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


