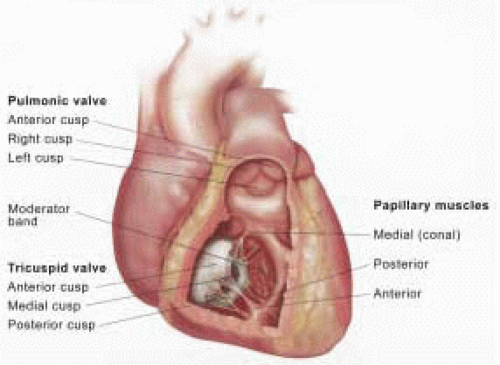
 FIGURE 16.1. Anatomic drawing of right ventricle with valves labeled, anterior view. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) |
annulus lies in a slightly more apical position than the mitral anulus, with its inferior margin near the entrances of the inferior vena cava and coronary sinus into the right atrium. The contribution of tricuspid annular motion to RV function is quite important. Downward or apical movement of the annulus significantly augments RV stroke volume, even more than the analogous movement of the mitral annulus. With loss of annular motion, systolic shortening of the RV free wall decreases substantially, significantly diminishing effective right heart function (2).
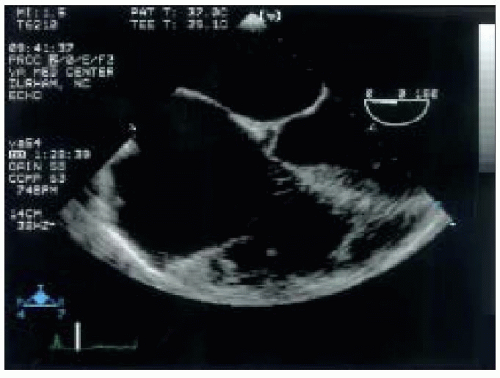 FIGURE 16.2. TEE of modified midesophageal four-chamber view showing the moderator band crossing the apical portion of the right ventricle. Note right atrial enlargement. |
aspect and across its transverse dimension (0, 30, and 60 degrees) to completely map the TR jet and determine the severity of regurgitation. Spectral Doppler examination of the valve may be attempted in this imaging plane, but the angle of interception between the direction of flow and the ultrasound beam may preclude an accurate result. The PV is not visualized in the ME 4-C view.
TABLE 16.1. Suggested Views for Imaging Tricuspid and Pulmonic Valves | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
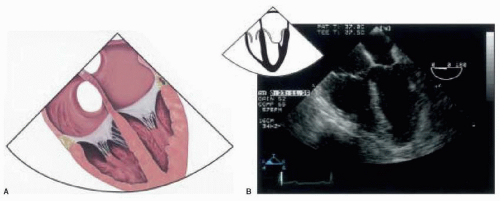 FIGURE 16.3 A: Anatomic drawing of the midesophageal four-chamber view. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) B: TEE of midesophageal four-chamber view with corresponding icon. |
tract (RVOT) (Figs. 16.4A and 16.4B). Rotation of the probe to the left (counterclockwise) may improve the image of the proximal main PA allowing evaluation of its first few centimeters for abnormalities. Of note, although the PV leaflets may not be clearly imaged in this view, CFD may still be used to detect pulmonic regurgitation (PR).
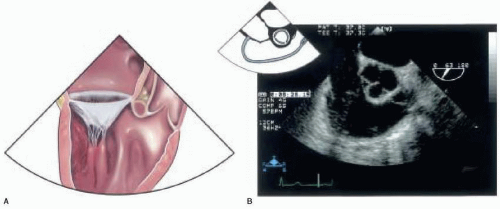 FIGURE 16.4. A: Anatomic drawing of right ventricular inflow-outflow view. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins, Figure 10.3.) B: TEE of right ventricular inflow-outflow view with corresponding icon. |
TV stenosis may be assessed using continuous wave (CW) Doppler techniques.
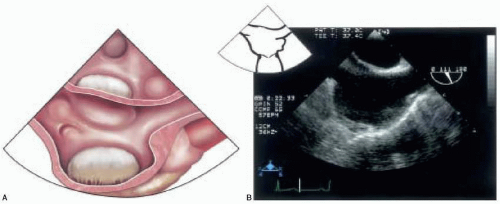 FIGURE 16.5. A: Anatomic drawing of bicaval view. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) B: TEE of bicaval view with corresponding icon. |
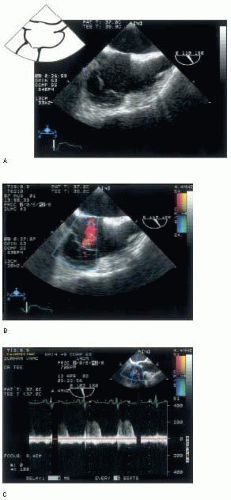 FIGURE 16.6. A: TEE of modified bicaval view with corresponding icon. B: Color Doppler of the tricuspid valve from the modified bicaval view. C: Spectral Doppler interrogation of the tricuspid valve. |
(Fig. 16.10). This scan plane provides the best view of the TV supporting structures, including the chordae tendinae and papillary muscles. The RV appears on the left, and the RA on the right of the display screen. From this scan plane, the TEE probe can be rotated further rightward (clockwise) to image the hepatic veins, most easily identified with CFD. Pulsed wave Doppler can then be used to evaluate hepatic flow patterns (Fig. 16.11). The PV and the RVOT can also be imaged from this probe location. From the TG RV inflow view at between 100 and 120 degrees, reducing the multiplane angle slowly toward zero and anteflexing brings the RVOT and the PV into view somewhere between 60 and 90 degrees (TG RV outflow view) (Fig. 16.12A) (7). At times, the aortic valve may appear just to the right of the PV, demonstrating the intimate relationship between the two semilunar valves (Fig. 16.12B).
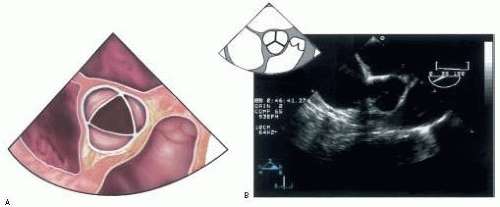 FIGURE 16.7. A: Anatomic drawing of midesophageal aortic valve short-axis view with right ventricular outflow tract seen. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) B: TEE of midesophageal aortic valve short axis with corresponding icon. |
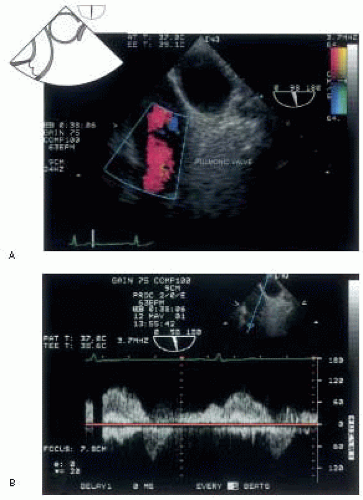 FIGURE 16.8. A: TEE of upper esophageal aortic arch short-axis view with color Doppler flow across the pulmonic valve. B: TEE of upper esophageal aortic arch short-axis view with spectral Doppler across the pulmonic valve demonstrating forward systolic flow and retrograde flow during diastole. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) |
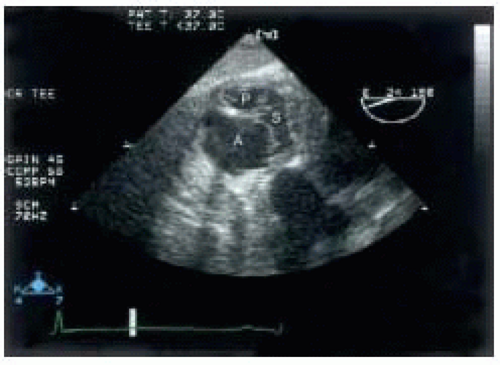 FIGURE 16.9. TEE of tricuspid valve short axis with leaflets labeled. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) |
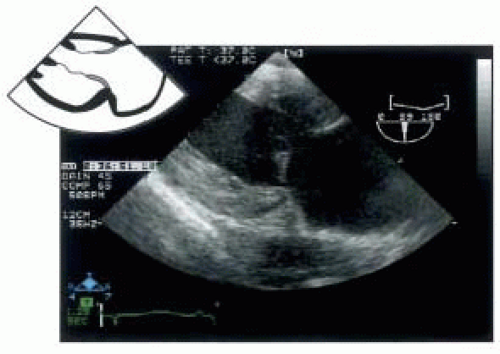 FIGURE 16.10. TEE of transgastric right ventricle view with corresponding icon. |
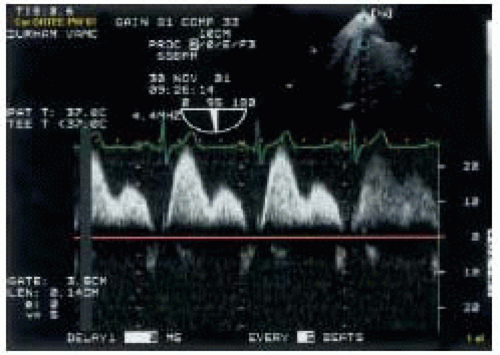 FIGURE 16.11. TEE of normal hepatic venous flow. |
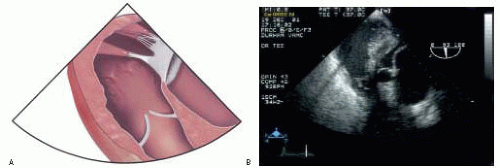 FIGURE 16.12. A: Anatomic drawing of transgastric right ventricular outflow view with pulmonic valve prominent. (Reprinted with permission from Konstadt SN, Shernan S, Oka Y, eds. Clinical Transesophageal Echocardiography: A Problem Oriented Approach, 2nd ed. Philadelphia: Lippincott Williams & Wilkins.) B: TEE of transgastric right ventricular outflow tract on the left and left ventricular outflow tract on the right. The aortic and pulmonic valves are clearly seen. |
 A) and restriction (E
A) and restriction (E  A) of RV filling. It is important to note that tricuspid inflow patterns have lower absolute
A) of RV filling. It is important to note that tricuspid inflow patterns have lower absolute velocities than the corresponding mitral inflow velocities owing to the lower pressures generated by the RV and the larger cross-sectional area of the TV.
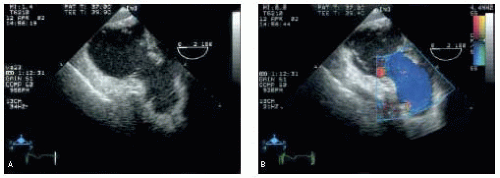 FIGURE 16.13. A: TEE of deep transgastric right ventricular outflow tract. B: TEE of deep transgastric right ventricular outflow view with color flow Doppler demonstrating transpulmonic flow. |
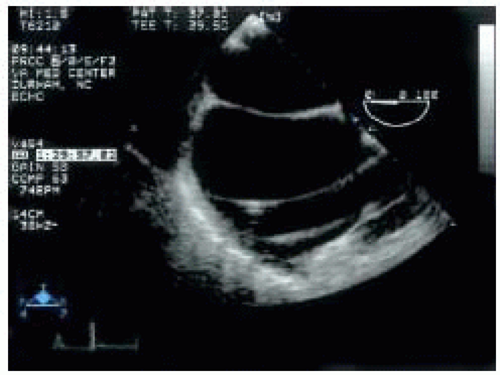 FIGURE 16.14. TEE focused on right atrium to demonstrate the pulmonary artery catheter echographic characteristics. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


