within the orifice as given by the hydraulic orifice formula (Fig. 22.1):
TABLE 22.1. Hemodynamic Data Obtainable with 2-D Doppler Echocardiography | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||
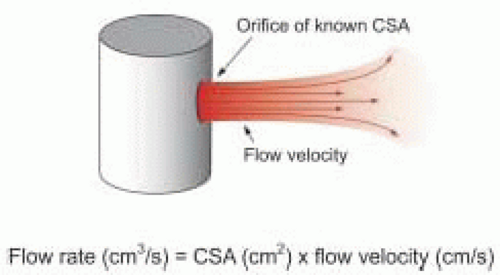 FIGURE 22.1. The hydraulic orifice formula. The volumetric flow rate through an orifice is equal to the product of the cross-sectional area of the orifice and the flow velocity of the fluid through the orifice. If flow velocity is constant, so is flow rate; however, if flow velocity varies, so will flow rate. CSA, cross-sectional area. |
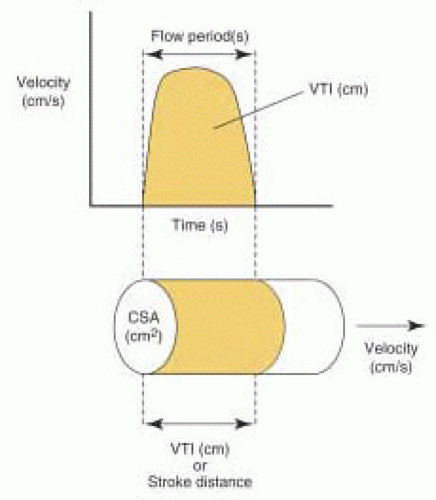 FIGURE 22.2. The Doppler velocity-time integral and stroke distance. As flow in the heart and great vessels is pulsatile, blood flow velocity varies during the period of ejection (or filling) as shown by the Doppler velocity curve. The area under the Doppler velocity curve (the velocity-time integral) is equivalent to the distance blood flow travels with one beat of the heart (stroke distance). VTI, velocity-time integral; CSA, cross-sectional area. |
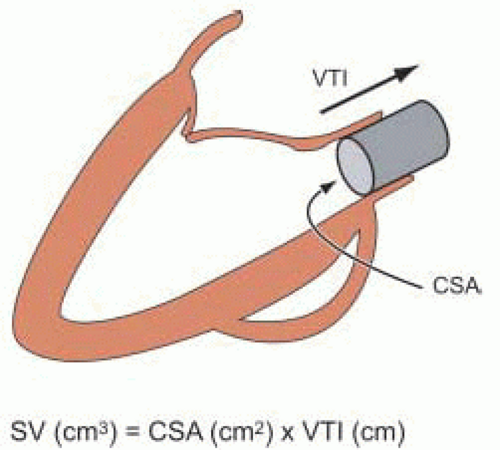 FIGURE 22.3. Doppler stroke volume calculation. The velocity-time integral of the Doppler velocity curve can be conceptualized as the length of a cylinder of blood (stroke distance) ejected through a cross-sectional area on one beat of the heart. Stroke volume is calculated as the product of cross-sectional area and the velocity-time integral. SV, stroke volume; CSA, cross-sectional area; VTI, velocity-time integral. |
TABLE 22.2. Assumptions for Accurate Doppler Stroke Volume Calculations | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
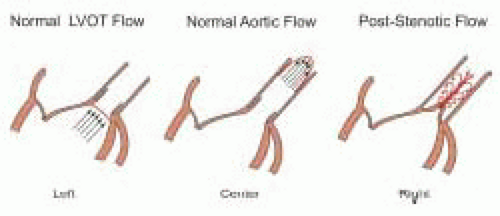 FIGURE 22.4. Common flow patterns. Left: Acceleration of blood within the left ventricular outflow tract leads to laminar flow with a flat velocity profile. Center: Friction along the wall of the ascending aorta leads to laminar flow with a parabolic flow profile. Right: Aortic stenosis results in a narrow, high velocity laminar jet originating from the stenotic orifice surrounded by turbulent flow. |
of the Doppler beam with blood flow. While underestimation of velocities is always a potential source of error in Doppler stroke volume determination with TEE imaging, it is undoubtedly less of a concern with multiplane than with monoplane or biplane TEE imaging.
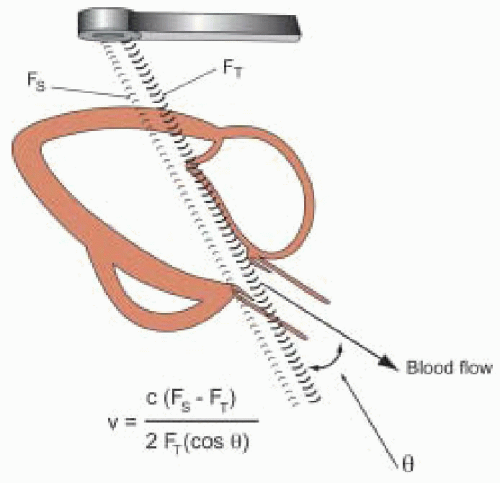 FIGURE 22.5. The Doppler equation. Blood flow velocity can be calculated based on the Doppler shift, which is the change in frequency between transmitted and backscattered ultrasound. v, blood flow velocity; c, the speed of sound in blood; FT, the frequency of transmitted ultrasound; FS, the frequency of backscattered ultrasound (the ultrasound reflected from moving red blood cells); θ, the angle between the blood flow and interrogating ultrasound beam. |
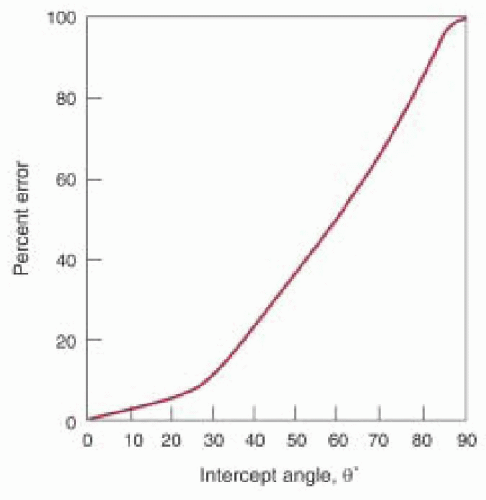 FIGURE 22.6. Velocity measurement error due to a nonparallel intercept angle. This graph shows the percentage error in the velocity calculation using the Doppler equation if the intercept angle between blood flow and the ultrasound beam is erroneously assumed to be zero. θ, the true angle between blood flow and the interrogating ultrasound beam. |
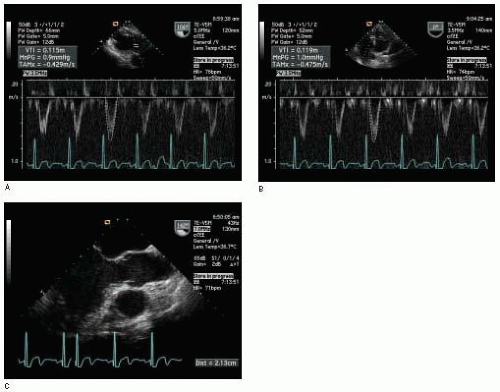 FIGURE 22.7. Data for LVOT stroke volume calculation. A: The VTILVOT can be measured using pulsed wave Doppler with the sample volume in the LVOT just proximal to the aortic valve from a transgastric long-axis view. B: Alternatively, the VTILVOT can be measured using pulsed wave Doppler with the sample volume in the LVOT just proximal to the aortic valve from a deep transgastric long-axis view. C: The diameter of the LVOT is usually measured from the midesophageal long-axis view of the aortic valve. VTI, velocity-time integral; LVOT, left ventricular outflow tract. |
from 80° to 90°) or the midesophageal short-axis view of the aorta for determination of the VTIPA. The diameter (cm) of the main pulmonary artery is obtained from either view at the same location for determination of the cross-sectional area using the formula for the area of a circle:
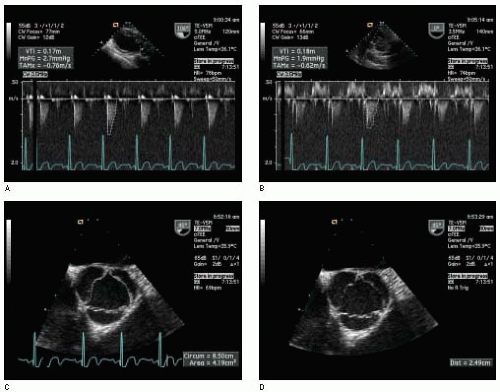 FIGURE 22.8. Data for transaortic valve stroke volume calculation. A: The VTIAV can be measured with the continuous wave Doppler beam placed through the aortic valve from a transgastric long-axis view. B: Alternatively, the VTIAV can be measured with the continuous wave Doppler beam placed through the aortic valve from a deep transgastric long-axis view. C: Planimetry can be used to measure the cross-sectional area of the aortic valve orifice during midsystole from a cine of the midesophageal short-axis view of the aortic valve. D: Alternatively, the length of a side of the aortic valve can be measured in midsystole for calculating the aortic valve area. VTI, velocity-time integral; AV, aortic valve; S, length of side of aortic valve. |
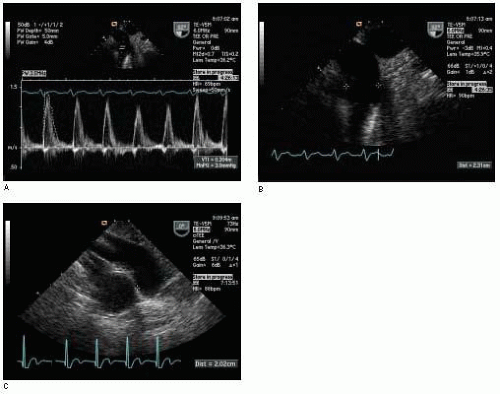 FIGURE 22.9. Data for main PA stroke volume calculation. A: The VTIPA can be measured using pulsed wave Doppler with the sample volume in the main pulmonary artery using the upperesophageal short-axis view of the aortic arch. B: The diameter of the main pulmonary artery can be measured from the same view at the same location. C: Alternatively, the diameter of the main pulmonary artery (as well as the VTIPA) can be measured using the midesophageal short-axis view of the ascending aorta (the VTIPA may also be obtained from this view). VTI, velocity-time integral; PA, pulmonary artery. |
the need for surgery or the timing of surgery. Qp/Qs can be calculated once the systemic stroke volume (measured at the LVOT or aortic valve) and pulmonic stroke volume (measured at the PA or RVOT) have been determined (14):
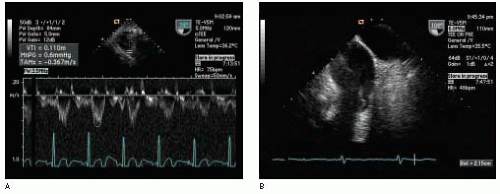 FIGURE 22.10. Data for RVOT stroke volume calculation. A: The VTIRVOT can be measured using pulsed wave Doppler with the sample volume placed just proximal to the pulmonic valve from a transgastric RV inflow-outflow view (transducer usually rotated from 110° to 150° and the probe turned to the right). B: The diameter of the RVOT may be obtained from this same view or the upper esophageal short-axis view of the aortic arch. VTI, velocity-time integral; RVOT, right ventricular outflow tract. |
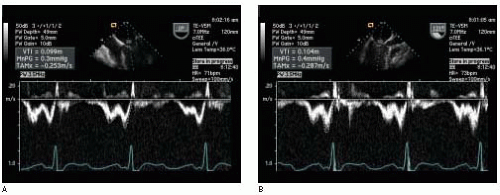 FIGURE 22.11. Data for transmitral stroke volume calculation. The VTIMV can be measured using pulsed wave Doppler with the sample volume placed within the mitral valve annulus using any midesophageal view of the mitral valve. A: The VTIMV measured from the midesophageal four-chamber view. B: The VTIMV measured from the midesophageal long-axis view in the same patient. (continued) |
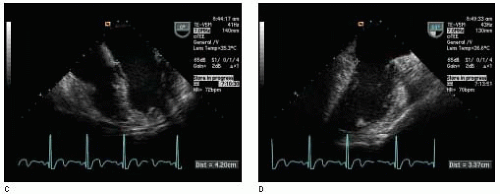 FIGURE 22.11. (Continued) C: The long diameter (D1) of the mitral valve annulus can be approximated using measurements from the midesophageal four-chamber view. D: The short diameter (D2) of the mitral valve annulus can be approximated using measurements from the midesophageal two-chamber view. VTI, velocity-time integral; MV, mitral valve. |
fraction. This potential propagation of errors will lead to a range in the confidence intervals for the mitral valve regurgitant volume, which is unacceptable to many clinicians. A particular problem exists with reliably measuring the mitral valve inflow stroke volume due to the irregular shape of the mitral valve orifice (semielliptical) and the fluctuation in its size during diastole (12). Furthermore, in the presence of significant aortic regurgitation this calculation is not accurate and mitral regurgitant volume will be underestimated.
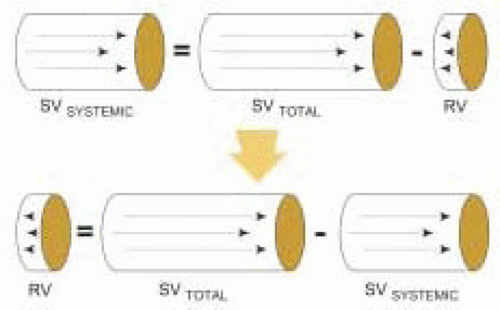 FIGURE 22.12. The volumetric method for calculation of regurgitant volume. Conservation of mass dictates that regurgitant volume must be equal to the difference between the total forward stroke volume across the regurgitant valve and the systemically delivered stroke volume. RV, regurgitant volume; SVTOTAL, total forward stroke volume across the regurgitant valve; SVSYSTEMIC, systemically delivered stroke volume. |
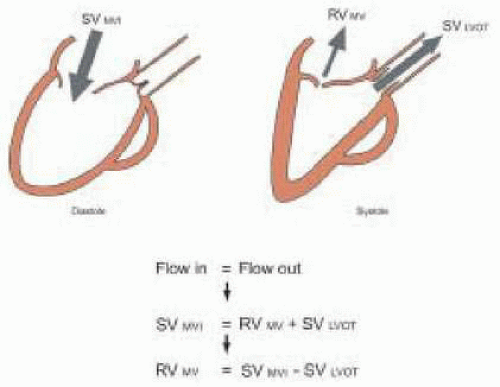 FIGURE 22.13. Assessment of mitral regurgitant volume using the volumetric method. Diastolic flow into the left ventricle must equal systolic flow out. Therefore, the mitral regurgitant volume must equal the difference between the mitral valve inflow stroke volume and the LVOT stroke volume. This method will underestimate mitral regurgitant volume in the presence of significant aortic regurgitation. RVMV, mitral regurgitant volume; SVMVI, mitral valve inflow stroke volume; SVLVOT, left ventricular outflow tract stroke volume. |
 FIGURE 22.14. Assessment of aortic regurgitant volume using the volumetric method. Diastolic flow into the left ventricle must equal systolic flow out. Therefore, the aortic regurgitant volume must be equal to the difference between the LVOT stroke volume and the mitral valve inflow stroke volume. This method will underestimate aortic regurgitant volume in the presence of significant mitral regurgitation. RVAV, aortic regurgitant volume; SVLVOT, left ventricular outflow tract stroke volume; SVMVI, mitral valve inflow stroke volume. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


