Viable means capable of living. One definition of myocardial viability is histological because viability is defined by the presence of living myocytes (1). During myocardial infarction viability is lost. A nonviable myocardium is one with infarcted (necrosed) tissue. Viable myocardium may be normal or dysfunctional in the reversible state of acute ischemia, stunning, or hibernation.
Myocardial Ischemia
As early as 1935, it was known that total ischemia stops myocardial contraction (2). Four abnormal contraction patterns develop in sequence: dyssynchrony—dissociation of adjacent segments in the course of contraction; hypokinesis; akinesis; and dyskinesis (3). The proportional decrease in regional myocardial blood flow and contractility is typical of acute myocardial ischemia (perfusion-contraction mismatch). Reperfusion within less than 10 minutes after coronary occlusion restores cardiac performance completely.
Myocardial Stunning
In the classic model of myocardial stunning, reperfusion after coronary occlusion lasting less than 15-20 minutes is associated with postischemic contractile dysfunction (4). Myocardial stunning is the fully reversible mechanical dysfunction that persists up to 24 hours after reperfusion despite restoration of normal or near-normal coronary blood flow (perfusion-contraction mismatch) (5,6,7). The severity of stunning is always greater in the subendocardial layers of the left ventricular wall than in the subepicardial layers (8). The diagnosis of stunning requires demonstration of two conditions: reversibility of the contractile abnormality and evidence of normal or near-normal coronary blood flow in the dysfunctional myocardium. Myocardial stunning is caused in part by injurious events during ischemia and reperfusion, so this contractile dysfunction can be considered a form of ischemia-reperfusion injury.
Hibernating Myocardium
Resting wall-motion abnormalities in patients with coronary artery disease (CAD) improve after administration of an inotropic agent (9). In 1978 Diamond et al. (10) introduced the concept of hibernating myocardium: Sometimes dramatic improvement in segmental left ventricular function after coronary artery bypass surgery suggested that the “ischemic non-infarcted myocardium can exist in a state of function hibernation.” In 1985, Rahimtoola (11) used the phrase hibernating myocardium to describe impaired ventricular function at rest because of reduced coronary blood flow that was restored when blood flow was improved or oxygen demand was reduced (12).
Myocardial hibernation can be defined as reversible left ventricular dysfunction due to chronic CAD (13). It is a complex, progressive, and dynamic phenomenon that is initiated by repeat episodes of ischemia. Patients with hibernating myocardium have normal or slightly reduced myocardial blood flow and limited coronary flow reserve. Hibernation involves repetitive postischemic dysfunction, perpetuated by renewed episodes of ischemia and changes in cell phenotype induced by ischemia-reperfusion, which eventually culminates in dramatic morphological alterations. Tissue necrosis is not substantial, although pathognomonic morphological changes have been found. A hibernating myocardium reveals residual contractile reserve with adrenergic stimulation. Regional and global ventricular function can improve in a hibernating myocardium after revascularization.
THE CLINICAL IMPORTANCE OF ASSESSING MYOCARDIAL VIABILITY
The assessment of myocardial viability in the perioperative setting has two applications:
To differentiate hibernating myocardium (reversible) from one with necrotic tissue (irreversible) for risk stratification and guidance of therapeutic decisions
To differentiate acute myocardial ischemia from stunning
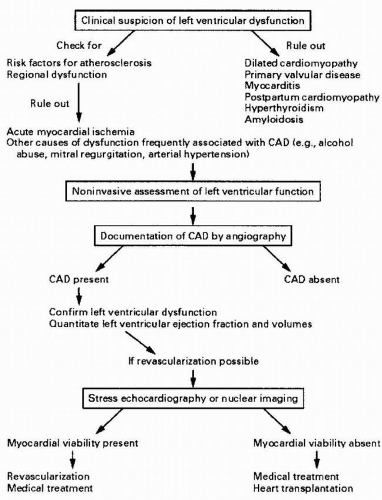
CAD is the most common cause of heart failure in the Western world, accounting for up to 60% of cases (14). Because of new therapeutic strategies that reduce the mortality associated with acute coronary syndromes, more patients suffer from the long-term sequelae of this condition. For many years, the functional sequelae of chronic CAD were considered irreversible and amenable only to palliative therapy; however, chronic left ventricular dysfunction is not necessarily caused by a myocardial infarction. It can be an effect of myocardial hibernation. The extent and severity of hibernating myocardium in patients with CAD varies considerably. The dysfunction may be limited to regional wall-motion abnormalities (RWMA) ranging from hypokinesia to akinesia or dyskinesia, with a relatively normal ejection fraction, or may involve global impairment of left ventricular function. In patients with CAD and no electrocardiographic evidence of previous myocardial infarction, prevalence of hibernating myocardium has been reported at 33% (15). Up to 50% of patients with a previous infarction may have areas of hibernating tissue mixed with areas of scar tissue, even in the presence of Q waves on the electrocardiogram (16). Noninvasive imaging to determine the presence and extent of viable myocardium distal to coronary stenoses is of considerable clinical importance because selection of patients for coronary revascularization depends on it (Fig. 23.1).
Coronary artery bypass graft (CABG) surgery contributes to improved regional and global left ventricular function in patients with left ventricular dysfunction with or without infarction (1722). In patients with CAD without previous myocardial infarction, revascularization is important both to reperfuse hibernating myocardium and to remove the source of repeated hypoperfusion. Of the asynergic myocardial segments that are revascularized, function will improve in 85% (23). In patients with CAD and previous myocardial infarction, functional recovery varies from 24% to 82% of segments (21). Recovery of function depends on a number of factors, including the severity of global left ventricular dysfunction preoperatively, the technique for myocardial protection during surgery, the presence or absence of perioperative myocardial infarction, and the adequacy of revascularization.
Revascularization is also associated with improved survival rates compared with medical therapy for patients with a left ventricular dysfunction caused by CAD (20,22,24,25). For patients with a left ventricular ejection fraction (LVEF) ≤ 35%, five-year survival rate for the surgical group was 68% compared with 54% for the group treated medically (20). In a surgical subgroup of patients with LVEF < 26%, five-year survival rate was 63% compared with 43% for the group treated medically (24,25,26,27,28). The results of surgical revascularization in patients with chronic left ventricular dysfunction is strongly affected by the presence of viable myocardium (15,29,30,31,32,33). After revascularization of a hibernating myocardium, improvement in the ejection fraction correlated with the number of dysfunctional but viable segments (34,35,36). Mortality was associated with a low-viability index; survival, both short- and long-term, was significantly better in patients with a high-viability index (6,16,22,37). Therefore, the presence of viable myocardium identifies patients most likely to benefit from coronary revascularization by postoperative improvement in LV systolic function, exercise capacity, quality of life, or survival. Identifying patients without viable myocardium is equally important in view of the high morbidity and mortality rates associated with surgery in such patients (38,39,40).
FIGURE 23.1. Algorithm for the identification of patients with hibernating myocardium. In addition to the evaluation of the viability of myocardial segments, the final choice of treatment is guided by many factors, such as coexisting conditions, age, and coronary anatomy. In most cases, medical treatment complements revascularization. CAD, coronary artery disease. With permission from Wijns W, Vatner SF, Camici PG. Hibernating myocardium. N Engl J Med 1998;339:173-81 (94).
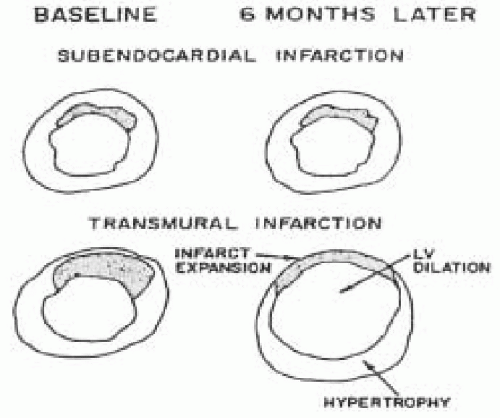
Reperfusion of viable myocardium may have beneficial effects other than improving LV function. With an admixture of scarred and viable myocardium (nontransmural infarct), reperfusion may not improve regional function. The presence of viable myocardium in the outer layers of the ventricular wall, however, maintains the left ventricular shape and size by preventing infarct expansion with subsequent heart failure (Figure 23.2) (41,42,43,44,45). A patent infarct-related artery reduces late mortality in patients after acute myocardial infarction independent of left ventricular systolic function (46,47,48,49). In addition, revascularization of nonsubendocardial tissue may reduce the likelihood of irritable electrical foci and arrhythmias, thereby reducing late mortality. Table 23.1 summarizes the implications of assessing myocardial viability in patients with chronic ischemic LV dysfunction.
Myocardial stunning, that is, reversible postoperative ventricular contractile dysfunction unrelated to a continuing source of ischemia, may follow CABG surgery (6). Distinguishing ventricular dysfunction caused by acute ischemia or infarction from stunned myocardium remains critical for determining perioperative management strategies (return to cardiopulmonary bypass, utilization of a mechanical assist device, administration of vasoactive drugs) and long-term prognosis (37,50,51). Improvement in regional function after an ischemic event or acute myocardial infarction may require days to weeks after the initial compromising episode, despite adequate restoration of coronary blood flow (52).
TABLE 23.1. Clinical and Economic Implications of Assessing Myocardial Viability in Patients with Chronic Ischemic Left Ventricular Dysfunction.
Presence of Viable Myocardium
Absence of Viable Myocardium
Clinical Implications
Advantage
Lower perioperative risk associated with PTCA or CABG
Improved LVSF after PTCA or CABG
Avoidance of PTCA or CABG in high-risk patients
Lower long-term cardiac morbidity and mortality after PTCA or CABG
Disadvantage
Higher long-term cardiac morbidity and mortality without PTCA or CABG
Higher perioperative risk associated with PTCA or CABG
Economic Implications
Lower cost with PTCA or CABG
Cost Savings
Lower costs for medical treatment after PTCA or CABG
Selective use of PTCA or CABG
Avoidance of heart transplantation
Cost Expenditures
Medical treatment of future cardiac complications
Treatment of perioperative complications or need for heart transplant
FIGURE 23.2. Relation between the transmurality of infarction and infarct expansion. A: There are fewer transmural infarcts because they are surrounded by normal myocardium, which will not expand, and the left ventricle will not dilate. B: In contrast, large infarcts, which have less normal tissue to buttress them, will expand and result in left ventricular (LV) dilation. With permission from Lindner JR, Kaul S. Assessment of myocardial viability with two-dimensional echo and magnetic resonance imaging. J Nucl Cardiol 1996;3:167-82 (41).
DIAGNOSTIC TECHNIQUES TO ASSESS MYOCARDIAL VIABILITY
A “bull’s-eye” model can describe the three-dimensional anatomy of an infarcted myocardium. Anatomically, the infarct zone at the center is surrounded by a border zone and normal myocardium in the outer zone. The border zone is thought to contain a mixture of infarcted and normal tissue, scattered in the form of “peninsulas” of infarcted myocardium in a “sea” of normal myocardium (53). The area of the infarct is confined within the vascular territory of the occluded coronary artery. The severity of ischemia is always maximal in the endocardial and minimal in the epicardial layer. Pathophysiologically, the severity of the injury is uniform, progressing from the center of the infarct laterally toward normally perfused tissue, except for an area at the lateral edge where overlapping portions of normally perfused and ischemic myocardium are mixed together.
Because assessing myocardial viability by histological methods is not practical, a number of diagnostic techniques are used. Diagnostic techniques are used to detect myocardial contractility, metabolic activity, or the persistence of microvascular integrity (Table 23.2). To differentiate hibernating from infarcted tissues and stunned from ischemic myocardium, the ideal imaging method should delineate infarcted from noninfarcted (viable) tissue and perfused from underperfused dysfunctional myocardium, respectively.
Serum markers, such as creatine kinase and troponin T or I, have limited value in the assessment of myocardial viability after an acute myocardial infarction. They are elevated only in the early period after an infarction and cannot localize the infarct territory. Assessment of myocardial viability with ECG is most helpful during an episode of chest discomfort to observe ST-segment elevation; otherwise ST-T abnormalities are not specific for a viable but ischemic myocardium. Resolution of ST-segment elevation can be helpful in determining successful reperfusion (54), but the absence of ST-segment resolution does not exclude reperfusion. ST-segment elevation resolves slowly in acute myocardial infarction even in the absence of reperfusion. The presence of Q waves on the ECG correlates poorly with the transmurality of infarction after successful reperfusion. The presence of Q waves does not rule out viable myocardium (55).
TABLE 23.2. Diagnostic Techniques for the Assessment of Myocardial Viability
Contractile Integrity
Metabolic Integrity
Microvascular Integrity
Echocardiography:
Electrocardiogram:
ST-segments, Q-waves
Myocardial contrast echocardiography:
Regional wall motion
Myocardial perfusion
Dobutamine
Thallium scintigraphy:
Myocardial perfusion and integrity of cell membranes
echocardiography:
Recruitable contractility
Positron emission tomography:
Myocardial metabolism and perfusion
Resting echocardiography assists in the assessment of both regional and global myocardial viability. Most left ventricular wall thickening occurs as a result of endocardial thickening; the middle layer of the myocardium contributes only modestly to thickening, and the contribution of the epicardium is negligible (56). In patients with CAD, a hypokinetic region at rest is a clue to viability. But whether hypocontractility is caused by acute ischemia, stunning, hibernation, or altered loading conditions cannot be determined. On the other hand, akinetic or dyskinetic segments are not necessarily nonviable. The overall contraction of a region after a myocardial infarction depends on how much subepicardial myocardium survives. When infarction involves < 20% of wall thickness, hypokinesia can be observed. When 20% of wall thickness is infarcted, akinesia or dyskinesia is seen (57). Thus, if the endocardium is necrosed, wall thickening is akinetic or even dyskinetic, but the middle and outer thirds of the ventricular wall may still be still perfused and viable (42,56).
Thallium scintigraphy is used to measure cell membrane integrity. The Na/K-ATPase system transports thallium like potassium across the myocyte sarcolemmal membrane. Cellular extraction of thallium across the cell membrane is unaffected in hypoxic, stunned, or hibernating myocardium, but thallium does not penetrate scarred tissue (58). Single-photon emission computerized tomography (SPECT) imaging at stress, redistribution (early and late), and reinjection at rest can assess myocardial viability. Assessment with technetium-99m sestamibi (Tc-99m MIBI) is still under active investigation. Positive and negative predictive accuracy for reversal of wall-motion abnormalities after revascularization varies, as do results after direct comparison with thallium scintigraphy.
Positron emission tomography (PET) imaging is regarded as the gold standard and final arbiter in decisions regarding viability (59). PET scanning tracks markers of perfusion (NH3) and metabolism of (18F-fluorodeoxyglucose) to compare blood flow and metabolism activity. Under normal conditions flow and metabolic activity match, and distribution of each tracer is homogeneous. Regional blood flow may be decreased while glucose utilization is normal or increased. This pattern of blood flow-metabolism mismatch signals myocardial viability in the presence of ventricular dysfunction. Decreases in blood flow and glucose utilization are a marker of myocardial scarring and irreversible damage. Measurement of myocardial blood flow by PET has several limitations, however. In the presence of spatial tissue heterogeneity with ischemic injury, the flow value may represent a transmural average between low values in necrotic areas to normal values in well-perfused zones. During flow restriction, subendocardial layers tend to have less flow than subepicardial layers. Therefore, a small reduction in average flow across the wall may correspond to a more severe reduction in subendocardial blood flow. Whether or not subendocardial blood flow is reduced in patients with hibernating myocardium awaits verification by direct measurement.
Dobutamine echocardiography and myocardial contrast echocardiography can be used in the operating room to differentiate hibernating myocardium from necrotic tissue and acute myocardial ischemia from stunning, respectively.
Dobutamine Echocardiography
Resting two-dimensional echocardiography cannot differentiate hibernating from irreversibly damaged myocardium because it does not account for coronary blood flow reserve. Provocative testing is necessary to find viable segments. Dobutamine echocardiography is a safe, noninvasive, and accurate diagnostic technique to identify viable myocardium in chronically dysfunctional regions (51,60,61,62,63,64). In the standard protocol for dobutamine stress echocardiography, increments of dobutamine from 5 to 40 µg/kg/min are added at three-minute intervals with intravenous atropine if 85% of the maximum predicted heart rate is not achieved. In a low-dose dobutamine protocol, which assesses left ventricular systolic function at baseline and at doses from between 5 and 10 µg/kg/min, the different contractile response in hibernating and infarcted myocardium distinguishes reversible from irreversible tissue injury.
Dobutamine is a synthetic catecholamine with strong β1-receptor and mild α1– and β2-receptor agonist activity (65). Dobutamine also may have a minor direct vasodilatative effect on coronary vessels. It has a plasma half-life of approximately 2 minutes and is metabolized rapidly by the liver.
Only gold members can continue reading. Log In or Register to continue