TABLE 35.1. Pathophysiology of Heart Failure—from Injury to Clinical Syndrome | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
chronic state of low perfusion that ends in multisystem failure and death unless adequate circulation is restored.
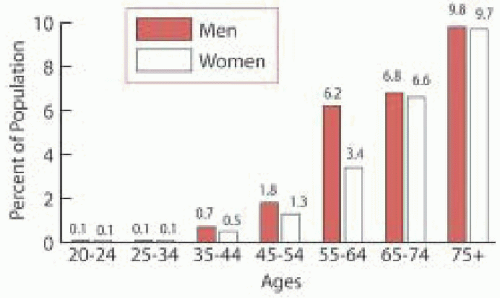 FIGURE 35.1. Prevalence of congestive heart failure by age and sex. Zoghbi WA, Enriquez-Sarano M, Foster E. et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr 2003;16(7):777-802. |
a rough measurement of LV systolic function with a normal range of 25% to 45%, using the following formula:
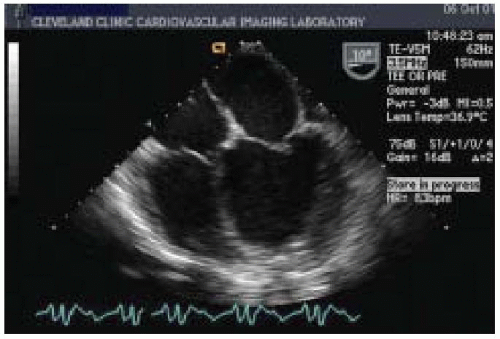 FIGURE 35.2. Dilated cardiomyopathy: midesophageal four-chamber view |
TABLE 35.2. Application of Intraoperative Echocardiography During Surgical Procedures for Congestive Heart Failure | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
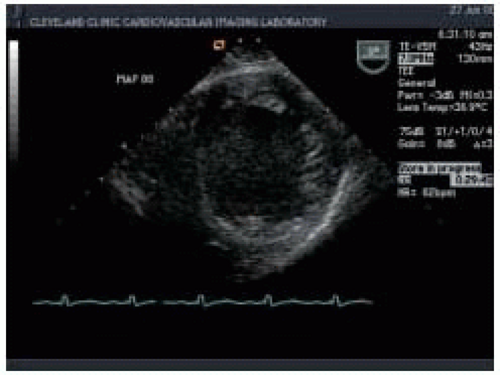 FIGURE 35.3. Dilated cardiomyopathy: transgastric midpapillary short-axis view |
TABLE 35.3. Typical Features of the Three Physiologic Types of Cardiomyopathy | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
careful echocardiographic assessment is mandatory if cardiopulmonary bypass is to be successful.
TABLE 35.4. Echocardiographic Approach to the Patient with a Suspected Cardiomyopathy | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
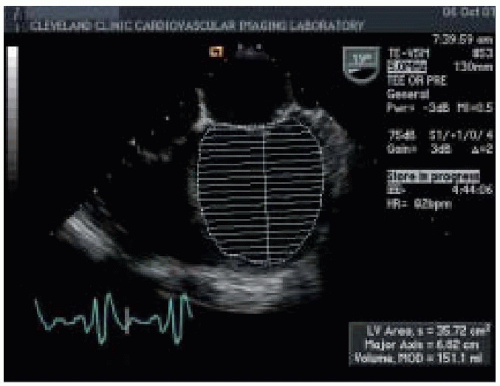 FIGURE 35.4. Dilated cardiomyopathy, left ventricle dimensions and volume: midesophageal four-chamber view |
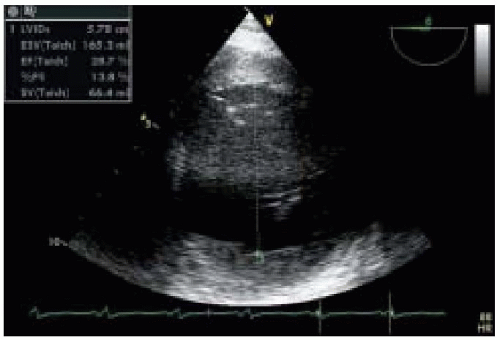 FIGURE 35.5. Dilated cardiomyopathy, left ventricle dimension and volume: transgastric short-axis midpapillary view |
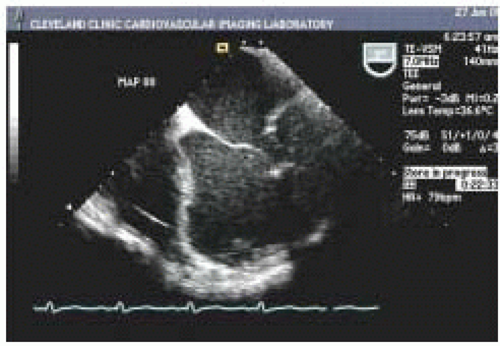 FIGURE 35.6. Left ventricular aneurysm: midesophageal four-chamber view |
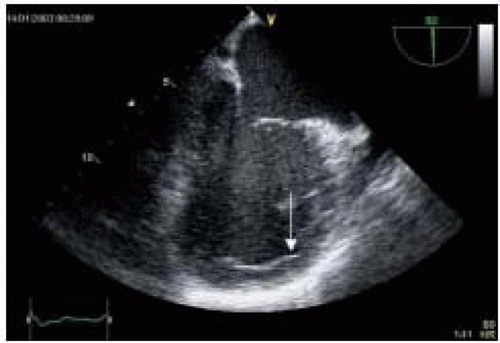 FIGURE 35.7. Ventricular thrombus: midesophageal two-chamber view |
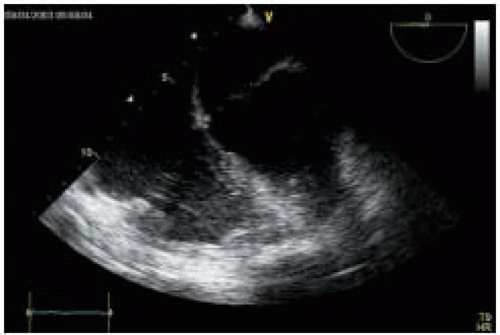 FIGURE 35.8. Biventricular failure: midesophageal four-chamber view |
(Table 35.5). Right ventricular SV and CO can be measured directly by imaging the RVOT tract and PA in the upper esophageal aortic arch short-axis (UE aortic arch SAX) view (Fig. 35.12). By measuring the diameter (D) of PA annulus and using PWD mode to determine velocity time integral (VTI) across pulmonic valve, right ventricular SV, and CO can be calculated using the formulas SV = PA D2 × 0.785 × PAVTI and CO = SV × HR.
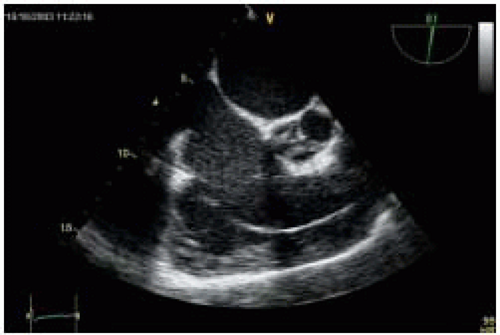 FIGURE 35.9. Right ventricular failure: midesophageal right ventricular inflow-outflow view |
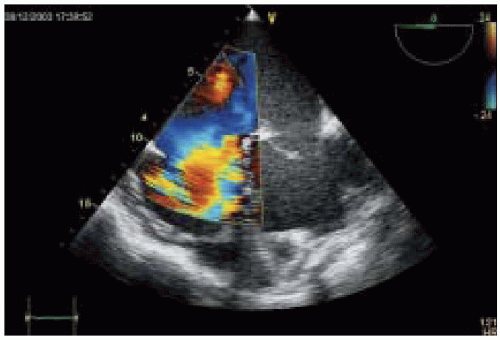 FIGURE 35.10. Severe tricuspid regurgitation: midesophageal four-chamber view |
TABLE 35.5. Estimation of Intracardiac Pressures | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
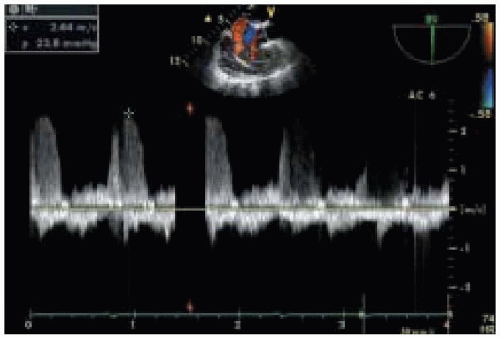 FIGURE 35.11. Tricuspid regurgitation, velocity, and pressure gradient |
CMP may report symptoms of heart failure despite normal EF, a condition known as diastolic heart failure (13,14). In addition, in patients with preexisting systolic dysfunction, abnormalities in diastolic dysfunction may be significantly related to the severity of cardiac symptoms and prognosis in patients with CHF (15). Diastole is the interval between aortic valve closure and mitral valve closure and can be divided into four phases:
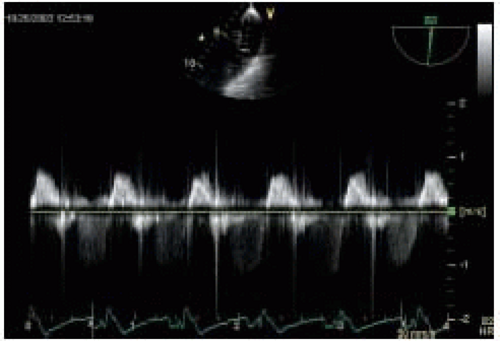 FIGURE 35.12. Pulsed wave Doppler of pulmonary artery |
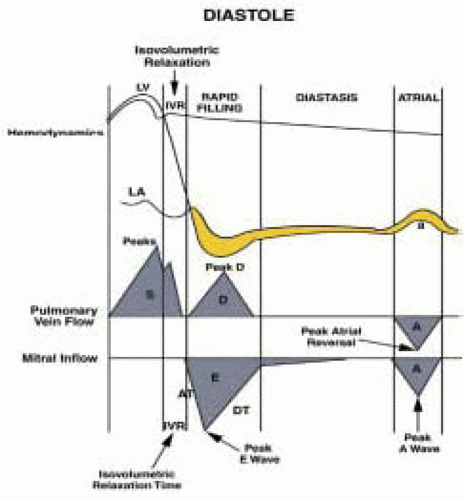 FIGURE 35.13. The relationship among left ventricular, left atrial, and aortic pressures |
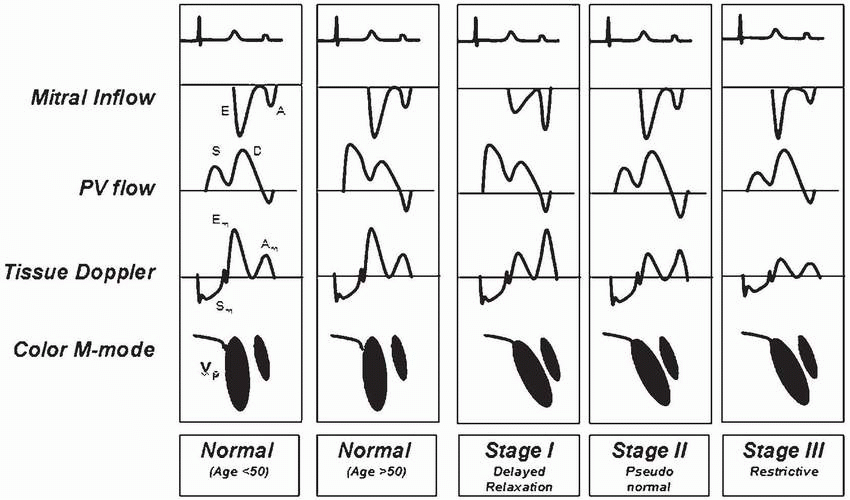
TABLE 35.6. Patterns of Diastolic Dysfunction | |
|---|---|
|
jet, if present. The ME 2-chamber view at 90° allows evaluation of the basal, mid, and apical segments of the anterior and inferior LV walls as well as examination of the left atrial appendage (LAA) for mural thrombi. The ME LAX view at 120 shows both basal and midanteroseptal segments, basal and midposterior segments, the left ventricular outflow tract (LVOT), and the aortic valve. The ME bicaval view is the image of choice for evaluating PFO by CFD and contrast study. This view provides information about the size of and blood flow through the RA, the left atrium (LA), and the right lower pulmonary vein (RLPV) using PW Doppler. TG views are obtained by advancing the probe into the stomach and flexing the tip anteriorly. TG basal and mid-SAX views are the views of choice for the examination of LV regional wall motion abnormalities. In addition, the TG basal SAX view provides a short-axis view of the MV that allows further location of the regurgitant jets using CFD. Rotating the multiplane angle 90° to the TG 2-chamber view allows further assessment of the LV anterior and posterior walls, the MV, and the LAA. The TG LAX view at 120° provides a longitudinal view of the AV and allows measurement of pressure gradients across the AV using continuous wave Doppler (CWD) and PWD. Turning the probe to the right and to 120° to the TG RV inflow view allows evaluation of the RV diaphragmatic and free walls, TV function, and RA dimensions. The deep TG LAX view provides a longitudinal view of the LV and AV and allows measurement of AV gradients and calculation of the AV area using CWD and PWD. Atherosclerotic disease in the descending aorta can be detected with the probe in a gastric position and the tip rotated posteriorly into the left descending aortic short-axis (descending aortic SAX) view. A longitudinal view of the descending aorta can be obtained at 90 in the descending aortic long axis (descending aortic LAX) view. The ME ascending aortic SAX/LAX views and upper esophageal (UE) aortic arch LAX/SAX views are used to examine the ascending aorta and should be used to guide cannulation and cross-clamping of the aorta. Doppler examination of the pulmonary valve is best achieved using the UE aortic arch SAX view (23).
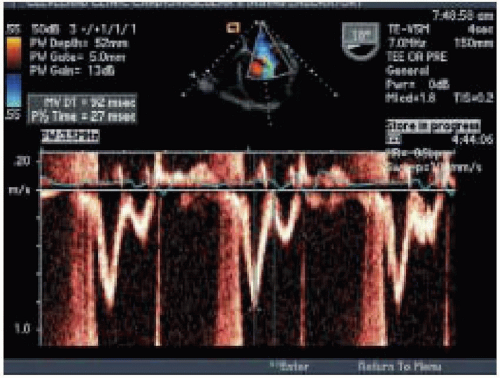 FIGURE 35.14. Pulsed wave Doppler: transmitral diastolic flow |
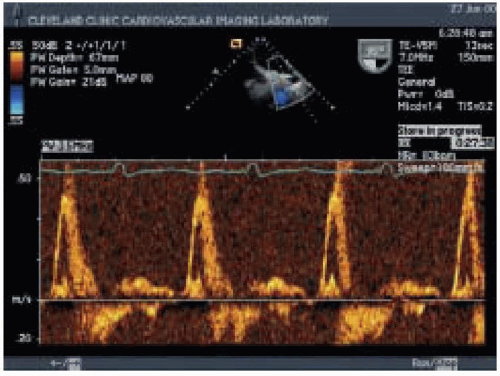 FIGURE 35.15. Left upper pulmonary vein pulse wave Doppler: restrictive pattern |
TABLE 35.7. Distinguishing the Patterns of Diastolic Dysfunction | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
RV end-diastolic volume (RVEDV), RV dP/dT, TV annulus diameter, and severity of TR is important. These parameters will allow comparison between baseline and postoperative RV performance and dictate postoperative management in the event of acute deterioration of RV function, which is often seen when respiratory insufficiency occurs.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


