7 Assessing Twist and Torsion
Background
Left Ventricular Systole
• Invasive parameters of LV systolic function during the IVC period include rate of change in pressure over time (dP/dt).
• LV stroke volume, ejection fraction (EF), and stroke work can be used to assess LV systolic function during the ejection phase.
• Apical rotation starts by an initial clockwise rotation during the IVC period, but the major rotation occurs during the ejection phase in a counterclockwise direction.
Left Ventricular Diastole
• During IVR, untwisting or recoil takes place and precedes LV expansion in the longitudinal and radial directions.
• An intraventricular pressure gradient follows untwisting, which helps direct LV intracavitary flow to the LV apex.
• This is followed by LV long axis expansion and mitral annulus early diastolic recoil velocity (e’).
• When the left atrial (LA) pressure exceeds LV diastolic pressure, the mitral valve opens and transmitral early diastolic velocity (E) is recorded.
Relation of Torsion to Cardiac Fiber Orientation
• Earlier activation of subendocardial fibers accounts for the apical clockwise rotation during IVC.
Definitions of Twist and Torsion
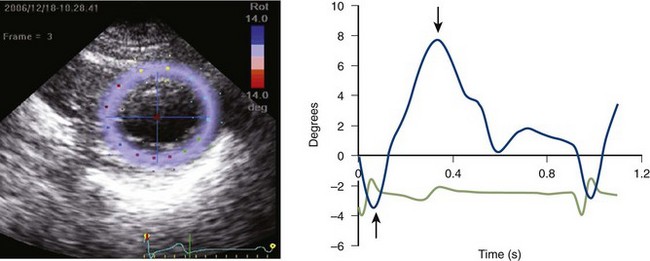
• Apical rotation starts with an initial clockwise movement followed by a net counterclockwise direction (positive sign) in normal hearts (Fig. 7-1).
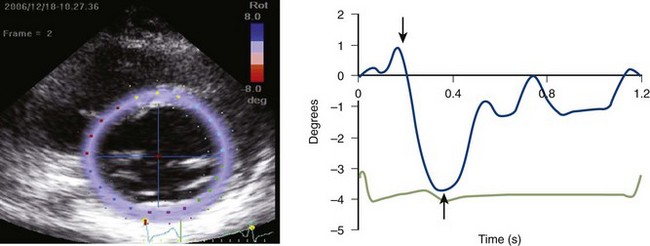
• Basal rotation starts with an initial counterclockwise movement followed by a net clockwise direction (negative sign) in normal hearts (Fig. 7-2).
• Twist varies with age and some studies have shown that it is higher in elderly subjects (>60 years).
• Torsion is the twist in degrees divided by LV long axis (distance between basal and apical segments).
• A better account of cardiac size is possible by calculating torsion as: Twist multiplied by average value of the radii of LV apical and basal cross sections divided by length.
• The above expression can allow comparison of rotational deformation between hearts of different sizes.
Definition of Untwisting
• Untwisting or recoil occurs during the isovolumetric relaxation time (IVRT) and early LV filling period.
• Peak untwisting velocity is usually measured and used to reflect the direction and speed of recoil.
• Aside from peak untwisting velocity, the timing of peak untwisting provides additional information.
Hemodynamic Determinants of Twist/Torsion
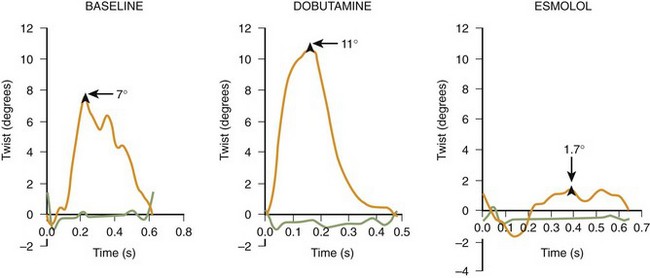
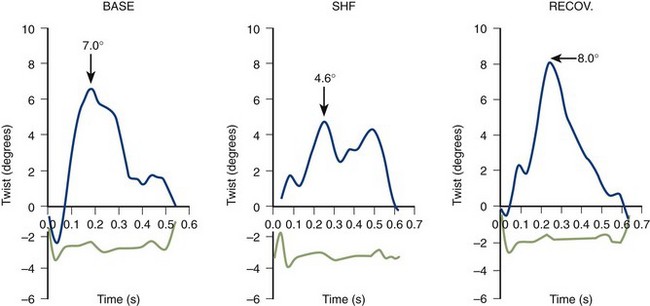
• An increase in LV contractility leads to an increase in torsion (Figs. 7-3 and 7-4). A direct positive correlation exists between torsion and LV EF, stroke volume, and dP/dt.
• In patients, simultaneous changes in load and contractility often occur and limit the clinical application of twist as a pure index of LV contractility.
Hemodynamic Determinants of Peak Untwisting Velocity
• An increase in LV twist leads to an increase in untwisting. This positive correlation occurs in normal and diseased hearts.
• The positive association between twist and untwisting was shown in animal experiments and human studies.
• A faster decline in LV pressure during IVRT, in the absence of a change in loading conditions, leads to an increase in LV peak untwisting velocity.
• In animal studies, dobutamine infusion was accompanied by shortening of tau and an increase in peak untwisting velocity.
• In animal studies, esmolol infusion was accompanied by prolongation of tau and a decrease in peak untwisting velocity.
• The impact of afterload on timing of untwisting was noted in patients with hypertrophic obstructive cardiomyopathy (HOCM).
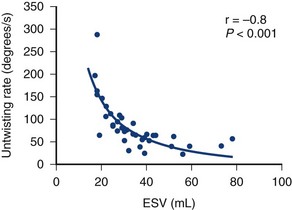
• In animal models, an acute increase in LV end-systolic volume leads to a decrease in untwisting velocity, despite unchanged LV relaxation. Conversely, an acute decrease in LV end-systolic volume leads to an increase in peak untwisting velocity in the absence of changes in LV relaxation (Fig. 7-5).
• In normal animals where load and contractility are both altered, peak untwisting velocity tracks best the changes in LV end-systolic volume.
• In patients with systolic heart failure, LV twist, time constant of LV relaxation, and LV end-systolic volume are the hemodynamic determinants of peak untwisting velocity.
• In patients with diastolic heart failure (DHF), LV twist and LV end-systolic volume (but not the time constant of LV relaxation) are the hemodynamic determinants of peak untwisting velocity.
Relation of Peak Untwisting to Left Ventricular Filling
• The above normal sequence is preserved in normal hearts with exercise, which leads to earlier onset of LV untwisting and therefore adequate LV filling despite higher heart rate and shorter diastolic filling time.
• With cardiovascular disease, the above sequence is disturbed such that peak LV untwisting can be delayed and may even follow mitral valve opening. This deprives the ventricle from the beneficial effects of untwisting on LV filling, which is maintained in these hearts by increased LA pressure.
• In patients with abnormal myocardial function, delayed untwisting is associated with increased LV filling pressures.
Effects of Exercise on Left Ventricular Twist Mechanics
• There are variations based on exercise type, intensity and duration, and whether measurements are obtained from elite athletes or not.
• After an ultra-long-distance triathlon, LV twist and untwisting can be reduced and delayed and accompanied by other indices of depressed LV systolic and diastolic function.
Key Points
• Apical rotation occurs in a net counter-clockwise direction when viewed from the apex (units: degrees).
Key Points
• In patients with systolic, and not diastolic, heart failure, a significant inverse correlation is present between the LV time constant of LV relaxation and peak untwisting velocity.
• Peak untwisting velocity occurs before mitral valve opening and helps maintain LV filling at low filling pressures.
Echocardiographic Approach (Table 7-1)
Acquisition
• Transducer frequency is 1.7 to 2 MHz; a higher frequency can be used in the absence of concerns for attenuation.
• TD can be of value when imaging patients with rapid heart rates, as in children and during exercise.
• TD has the limitation of a low signal-to-noise ratio and is heavily dependent on the presence or absence of angulation between the ultrasound beam and the plane of motion.
• The above limitations of TD have limited its application for the objective of measuring torsion and untwisting.
• Speckle tracking echocardiography (STE) is the most practical technique to measure torsion at this time.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


