Aspiration Pneumonia
Timothy C. Allen MD, JD
Roberto Barrios MD
Abida Haque MD
Philip T. Cagle MD
Aspiration pneumonia in adults occurs generally from the aspiration of particulate gastric contents in elderly or disabled patients, the perioperative aspiration of gastric contents, and the aspiration of enteric solutions or other inhaled or locally applied oils (lipoid pneumonia, also termed exogenous lipid pneumonia). Aspiration pneumonia in children often involves foreign body aspiration or aspiration of oils or similar materials such as milk, resulting in lipoid pneumonia. Occasionally, aspiration of charcoal or barium solution occurs. Aspiration pneumonia may also be a complication of radiotherapy or chemotherapy to the head and neck or, in patients with diabetes mellitus, as a complication of diabetic gastroparesis.
Histologically, aspiration pneumonia acutely consists of pulmonary edema and congestion, atelectasis, and alveolar epithelial cell necrosis, with an intense neutrophilic infiltrate occurring in 4 to 5 hours. Hyaline membrane formation occurs within 1 to 2 days, and transbronchial biopsy may be performed during this period, suggesting diffuse alveolar damage. A limited transbronchial biopsy may contain any mixture of these features and may be nonspecific. Depending on the circumstances, bacterial clusters, foreign body macrophages, granuloma formation, or foreign material may be present on the transbronchial biopsy. Lipoid pneumonia typically shows collections of foamy, lipid-laden macrophages lying within the alveolar spaces as well as within alveolar septa. In patients with ongoing chronic aspiration, septal fibrosis may be present.
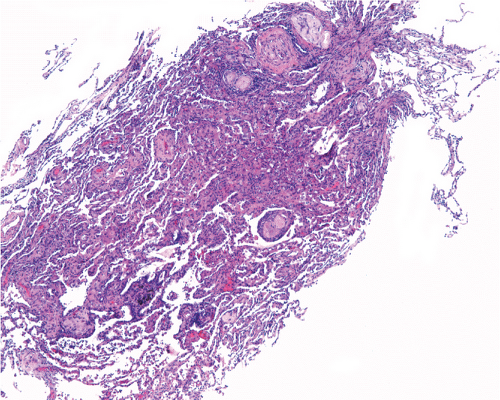 Figure 20.1: Low power of transbronchial biopsy from patient with chronic aspiration shows areas of interstitial pneumonia with fibrosis and chronic inflammation around fragments of foreign material.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|