Whenever a patient with an abnormal chest radiograph is evaluated, the possibility of a pleural effusion should be considered. Increased densities on the chest radiograph are frequently attributed to parenchymal infiltrates when they actually represent pleural fluid. Most patients with pleural effusions have blunting of the posterior costophrenic sulcus on the lateral chest radiograph. If this angle is blunted, the patient should be evaluated with ultrasound, CT scan, or bilateral decubitus chest radiographs to ascertain whether free pleural fluid is present (see Chapter 6). This chapter provides a guide to the approach to a patient with an undiagnosed pleural effusion. The British Thoracic Society has recently published guidelines for the investigation of a unilateral pleural effusion in adults (1). The management of patients with pleural effusions due to specific diseases is discussed in the chapters dealing with those diseases.
FREQUENCIES OF VARIOUS DIAGNOSES
Pleural effusions can occur as complications of many different diseases (Table 8.1). The vigor with which various diagnoses are pursued depends on the likelihood that the individual has that particular disease. Table 8.2 shows the approximate annual incidence for the most common causes of pleural effusions. An epidemiologic study from the Czech Republic found that the four leading causes of pleural effusions in order of incidence were congestive heart failure, malignancy, pneumonia, and pulmonary embolism (2). Congestive heart failure and cirrhosis cause almost all transudative pleural effusions, whereas malignant disease, pneumonia, and pulmonary embolization are the three main causes of exudative pleural effusions. Two other frequent causes of exudative pleural effusions are viral infections and the effusion that occurs after coronary artery bypass graft (CABG) surgery.
SEPARATION OF EXUDATES FROM TRANSUDATES
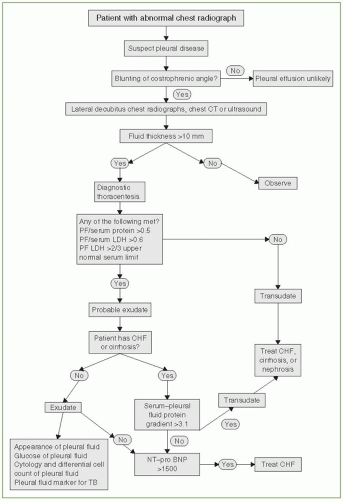
If free pleural fluid is demonstrated on the decubitus film, with ultrasound or with a CT scan, one should consider performing a diagnostic thoracentesis (Fig. 8.1). It has been my experience that diagnostic thoracentesis is difficult if the thickness of the fluid on the decubitus radiograph, ultrasound, or the CT scan is less than 10 mm. If the thickness of the fluid is greater than 10 mm, however, consideration should be given to performing a diagnostic thoracentesis (see Chapter 28). If the patient has obvious congestive heart failure, I perform a diagnostic thoracentesis if any of the following three conditions are met: (a) the effusions are not bilateral and comparably sized, (b) the patient has pleuritic chest pain, or (c) the patient is febrile. Otherwise, treatment of the congestive heart failure is initiated. If the pleural effusions do not rapidly disappear, I then perform a diagnostic thoracentesis several days later. It must be remembered, however, that the characteristics of the pleural fluid may change from those of a transudate to those of an exudate with diuresis. Romero et al. (3) performed a thoracentesis on 15 patients with congestive heart failure before and every 48 hours after diuretic therapy was initiated. Before diuretics were administered, only one effusion was misclassified as an exudate by Light’s criteria, but at the time of the third thoracentesis 10 effusions were misclassified as exudates. Between the first and the third thoracentesis, the mean protein level increased from 2.3 to 3.5 g/dL and the mean lactate dehydrogenase (LDH) level increased from 176 to 262 IU/L (3).
TABLE 8.1 ▪ Differential Diagnosis of Pleural Effusion
Transudative pleural effusions
Congestive heart failure
Cirrhosis
Nephrotic syndrome
Superior vena caval obstruction
Urinothorax
Peritoneal dialysis
Glomerulonephritis
Myxedema
Cerebrospinal fluid leaks to pleura
Hypoalbuminemia
Sarcoidosis
Exudative pleural effusions
Neoplastic diseases
Metastatic disease
Mesothelioma
Body cavity lymphoma
Pyothorax-associated lymphoma
Infectious diseases
Bacterial infections
Tuberculosis
Fungal infections
Parasitic infections
Viral infections
Pulmonary embolization
Gastrointestinal disease
Pancreatic disease
Subphrenic abscess
Intrahepatic abscess
Intrasplenic abscess
Esophageal perforation
Postabdominal surgery
Diaphragmatic hernia
Endoscopic variceal sclerosis
Postliver transplant
Heart diseases
Postcoronary artery bypass graft surgery
Postcardiac injury (Dressler’s) syndrome
Pericardial disease
Post-Fontan procedure
Pulmonary vein stenosis postcatheter ablation of atrial fibrillation
Obstetric and gynecologic disease
Ovarian hyperstimulation syndrome
Fetal pleural effusion
Postpartum pleural effusion
Meigs’ syndrome
Endometriosis
Collagen vascular diseases
Rheumatoid pleuritis
Systemic lupus erythematosus
Drug-induced lupus
Sjögren’s syndrome
Familial Mediterranean fever
Churg-Strauss syndrome
Wegener’s granulomatosis
Drug-induced pleural disease
Nitrofurantoin
Dantrolene
Methysergide
Ergot drugs
Dasatinib
Amiodarone
Interleukin 2
Procarbazine
Methotrexate
Clozapine
Miscellaneous diseases and conditions
Asbestos exposure
Postlung transplant
Postbone marrow transplant
Yellow nail syndrome
Sarcoidosis
Uremia
Trapped lung
Therapeutic radiation exposure
Drowning
Amyloidosis
Milk of calcium pleural effusion
Electrical burns
Extramedullary hematopoiesis
Rupture of mediastinal cyst
Acute respiratory distress syndrome
Whipple’s disease
Iatrogenic pleural effusions
Hemothorax
Chylothorax
One of the main purposes of the diagnostic thoracentesis is to determine whether the patient has a transudative or an exudative pleural effusion. This distinction is made by analysis of the levels of protein and LDH in the pleural fluid and in the serum (4). If none of the criteria in Figure 8.1 is met, the patient has a transudative pleural effusion. Therefore, the pleural surfaces can be ignored while the congestive heart failure, cirrhosis, or nephrosis, for example, is treated. Alternately, if any of the three criteria in Figure 8.1 is met, the patient probably has an exudative pleural effusion. The exudative nature indicates that the pleural effusion resulted from local disease where the fluid originated, and further investigation should be directed toward the genesis of the local disease (5). It should be remembered, however, that 15% to 20% of patients with congestive heart failure or cirrhosis will meet Light’s criteria for exudative effusions. This is particularly likely if the patient has been receiving diuretics before the thoracentesis (6). If a patient has congestive heart failure or cirrhosis but the pleural fluid meets exudative criteria, the difference between the serum protein and pleural fluid protein (the pleural fluid protein gradient) should be measured. If this difference exceeds 3.1 g/dL, the patient should be classified as having a transudative pleural effusion and no further diagnostic tests are indicated (3). Alternatively, if the pleural fluid or serum NT-pro-BNP is greater than 1,300 pg/ml, the patient most likely has congestive heart failure (7).
TABLE 8.2 ▪ Approximate Annual Incidence of Various Types of Pleural Effusions in the United States
Congestive heart failure
500,000
Parapneumonic effusion
300,000
Malignant pleural effusion
200,000
Lung
60,000
Breast
50,000
Lymphoma
40,000
Other
50,000
Pulmonary embolization
150,000
Viral disease
100,000
Cirrhosis with ascites
50,000
Postcoronary artery bypass graft surgery
50,000
Gastrointestinal disease
25,000
Tuberculosis
2,500
Mesothelioma
2,300
Asbestos exposure
2,000
If there is a significant likelihood that the patient has a transudative pleural effusion, the most cost-effective utilization of the laboratory is to only obtain the protein and LDH levels of the pleural fluid at the initial diagnostic thoracentesis. Pleural fluid can be set aside for other tests if the fluid proves to be an exudate. Peterman and Speicher (8) reviewed the charts of 83 patients whose pleural fluid was a transudate by protein and LDH levels during a 1-year period. They found that 725 additional studies were performed on these 83 pleural fluids. Only 9 of the 725 studies yielded a positive result, and the positive result was eventually proved to be false in seven of the nine instances. If no tests other than the protein and LDH had been obtained in these 83 patients, there would have been a mean cost savings of US$185 per patient.
DIFFERENTIATING AMONG VARIOUS EXUDATIVE PLEURAL EFFUSIONS
To differentiate among the various causes of exudative pleural effusions, one should initially examine the gross appearance of the fluid, obtain a pleural fluid differential cell count and cytologic examination, measure the levels of glucose and LDH in the pleural fluid, and obtain a test for a pleural fluid marker for tuberculosis. Other tests can then be ordered on an individual basis.
Appearance of Pleural Fluid
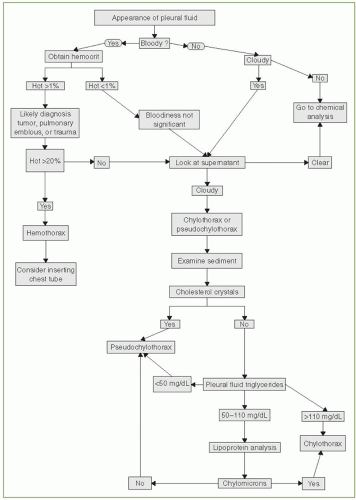
The gross appearance of the pleural fluid should always be noted and evaluated as outlined in Figure 8.2. If the pleural fluid appears bloody, a hematocrit should be obtained on the fluid. The hematocrit is frequently much lower than would be expected from the appearance of the pleural fluid. The blood in the pleural fluid is not significant if the pleural fluid hematocrit is less than 1% (9). If the pleural fluid hematocrit is greater than 1%, the patient most likely has malignant pleural disease, a pulmonary embolus, or a traumatically induced pleural effusion (9). If the hematocrit is greater than 50% of that of the peripheral blood, the patient has a hemothorax, and one should consider performing a tube thoracostomy (see Chapter 25).
Many laboratories are hesitant to perform hematocrits on pleural fluid and rather report a red blood cell (RBC) count. These RBC counts are often inaccurate because the counts are not done with an automated counter and laboratory personnel are not always adept at determining RBC counts in body fluids that are bloody. Nevertheless, if the RBC count is obtained and is accurate, one can get a good estimation of the hematocrit in the pleural fluid by dividing the RBC count by 100,000. For example, a RBC count of 1,000,000 correlates with a hematocrit of 10.
If the pleural fluid is turbid or milky or if it is bloody, the supernatant of the pleural fluid should be examined to see whether it is cloudy. If the pleural fluid was turbid when originally withdrawn, but the turbidity clears with centrifugation, it was due to cells or debris in the pleural fluid. Most patients who have very turbid pleural fluid that clears with centrifugation have a pleural infection. If the turbidity persists after centrifugation, the patient probably has a chylothorax or a pseudochylothorax (see Chapter 26). These two entities can be differentiated by the patient’s history, examination of the sediment for cholesterol crystals, and lipid analysis of the supernatant (Fig. 8.2). Pseudochylothoraces usually occur when the pleural effusion has been present for many years. Cholesterol crystals may be found in the sediment, and high levels of triglycerides are not usually present in the pleural fluid. In contrast, chylothoraces are more acute, do not contain cholesterol crystals, and are characterized by high levels of triglycerides. The management of a patient with a chylothorax or a pseudochylothorax is discussed in Chapter 26.
FIGURE 8.2 ▪ Algorithm for evalating the appearance of pleural fluid. Hct, hematocrit.
Routine Measurements on Exudative Pleural Fluids
When a patient has an undiagnosed exudative effusion, there are several tests that should be routinely obtained, namely, a pleural fluid cell count and differential, a pleural fluid glucose and LDH level, examination of the pleural fluid for malignant cells, and a pleural fluid marker for tuberculosis (10). A good starting point for the diagnostic assessment of an unknown exudate is the pleural fluid cytology. An algorithm starting with the pleural cytology is presented in Figure 8.3.
In previous editions of this book, I recommended that a pleural fluid amylase also be obtained. However, the pleural fluid amylase only helps occasionally in making a diagnosis and, therefore, it should not be obtained on a routine basis (11). It should be obtained if acute pancreatitis, esophageal rupture, or chronic pancreatic pleural effusion is suspected (11).
Only gold members can continue reading. Log In or Register to continue