Fig. 17.1
The aortic valve annulus is measured by aortography in posterior-anterior projection. The double-headed arrow indicates the aortic annulus diameter between the hinge points of the valve leaflets

Fig. 17.2
Echocardiographic measurement of the aortic valve annulus between the hinge points of the valve leaflets (double-headed arrows) in the parasternal long-axis view
4.
Select the appropriate balloon: Balloon valvuloplasty-induced aortic regurgitation can be the result of commissural avulsion and cusp tear or perforation. It can make further surgical reinterventions more difficult. Oversized balloons are a risk factor for aortic regurgitation. The balloon-to-annulus ratio should be less than 1:1. Start with a balloon diameter of about 80 % of the aortic annulus and increase its size by 1 mm.
Concerning length, an ideal balloon length should allow safe straddling of the aortic valve without overlapping the mitral valve chordae. We often choose a 20-mm balloon length in newborns and 30 mm in older children and 40 mm in adolescents.
5.
Techniques of valvuloplasty: The techniques of valvuloplasty include single- and double-balloon valvuloplasty.
5.1.
Single-balloon valvuloplasty technique: With the help of an angiographic catheter (Judkins right, multipurpose catheter), cross the stenotic aortic valve by using a hydrophilic guidewire (0.014″ standard coronary wires in neonates, 0.018″ hydrophilic J-tipped wires in small kids, 0.035″ J-tipped wires in older kids and adolescents). Special care should be paid to avoid any force applied by the wire over the aortic cusps. Another important point is to be sure that you are not in the coronary artery with the wire.
The angiographic flow jet on the ascending aortogram may be used as a guide.
Exchange the hydrophilic wire for another wire (0.014″ coronary wire in newborns, 0.035″ standard guidewire in children, J-tipped 0.035″ extrastiff guidewire in adolescents) that will be used for the angioplasty. The wire is placed in the LV apex along the septum, anterior to the mitral valve chordal apparatus.
Advance a balloon valvotomy catheter over the guidewire, straddle the valve into the correct position, and inflate with a pressure of 4–7 ATM until the balloon waist disappears (Fig. 17.3). In newborns hand inflation is enough. Each inflation-deflation period lasts no more than 5–10 s. To preserve balloon stability across the aortic valve during inflation, a technique called temporary rapid pacing arrests mechanical systole to decrease the chance of balloon migration. The technique is performed by putting a bipolar pacing catheter in the right ventricular apex and using VVI pacing at a rate of 220–240 impulses per minute during the balloon inflation. Ultimately, such pacing can increase the success rate of the procedure.

Fig. 17.3
Single-balloon technique in posterior-anterior projections
5.2.
Double-balloon valvuloplasty technique: Except for the use of two separate arterial catheters to cross the aortic valve retrograde, the double-balloon technique is identical to the single-balloon approach. Each balloon has a similar diameter and length so the ratio of the sum to the valve annulus diameter is about 1:3. The two balloons are positioned similarly across the aortic valve and inflated simultaneously (Fig. 17.4). Studies [1] have suggested that the double-balloon valvuloplasty technique provides improved gradient relief by producing deeper tears in the lines of commissural fusion than can be obtained with a single balloon. In addition, two smaller balloons can be introduced to and removed from the femoral arteries more easily and, presumably, with less vessel trauma than a single large balloon. Third, the double-balloon technique extends the range of annulus sizes amenable to balloon dilation. It allows effective dilation of an aortic annulus ≤31 mm in diameter. Finally, inflation of two smaller balloons side by side has a smaller risk of completely occluding left ventricular outflow than inflation of a single larger balloon.
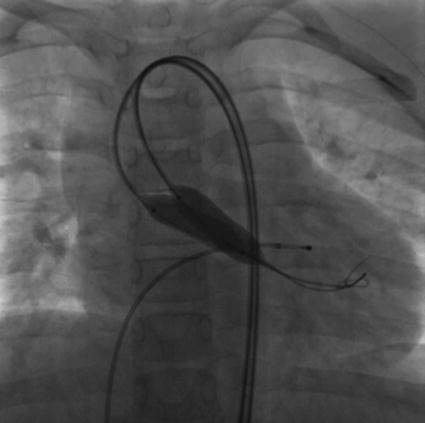
Fig. 17.4
Double-balloon technique in posterior-anterior projections
6.
Postoperative evaluation: Hemodynamic assessment is conducted again using angiography and echocardiography. The ideal surgical result is effective relief of stenosis (residual gradient < 30 mmHg) without moderate to severe aortic regurgitation.
17.7 Materials
Different balloon and guidewire products are available:
1.




Tyshak and Tyshak II (NuMED, Inc.) are often used in aortic valvuloplasty. Except for the balloon diameters of 21 and 24 mm, they provide a wide range of balloon diameters, from 4 to 30 mm, with 1-mm increments up to 25 mm. Because it has a thicker shaft and wire, Tyshak can better resist the left ventricular ejection power and is therefore preferred in older children. On the other hand, Tyshak II is preferable in infants in whom the lowest possible introducer profile is important. Tyshak Mini usually applies to neonates; it provides balloon diameters between 4 and 10 mm and needs introducer sizes of only 3–4 Fr. But it can only be guided by 0.014-in. wires.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
