Aortic Insufficiency
Allen P. Burke, M.D.
Fabio R. Tavora, M.D., Ph.D.
Etiology
In the previous century, aortic insufficiency was most commonly secondary to postinflammatory (rheumatic) valve disease. Postinflammatory fibrosis causes retracted and incompetent leaflets that are stiff and scarred, resulting in a component of stenosis. Pure aortic insufficiency is caused by infectious endocarditis with perforation of a leaflet (Chapter 177), dilated aortic root with lack of coaptation of the leaflets during diastole, and prolapse of one or more leaflets, often with myxoid or “floppy” change. Bicuspid valve can lead to isolated prolapse, is associated with aortic aneurysms, and is therefore overrepresented in not only aortic stenosis but also aortic insufficiency.
The 4 anatomic causes of aortic incompetence are therefore cusp retraction (chronic rheumatic disease), cusp perforation (endocarditis or trauma), cusp prolapse (myxomatous valve), and lack of coaptation or “diastasis” (dilated aortic root) (Table 173.1).
In a classic series of valve resections reported in 1984, the most common causes of aortic regurgitation were postinflammatory disease (46%), aortic root dilatation with or without bicuspid valve (21%), incomplete closure of a congenitally bicuspid aortic valve with normal aortic root (20%), infective endocarditis (9%), and other (4%).1
TABLE 173.1 Causes of Aortic Insufficiency | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
Since the 1980s, the prevalence of rheumatic valve disease has decreased, and the incidence of aortic aneurysm has increased. A more recent study of 107 purely insufficient resected valves the causes to be ascending aortic aneurysm with trileaflet valve (34%), aortic prolapse of trileaflet valve without aortic aneurysm (31%), aortic aneurysm with bicuspid valve (19%), bicuspid valve with prolapse and normal aortic root (12%), and postinflammatory aortic insufficiency (5%)2 (see Chapter 35). The types of aneurysms were most commonly due to medial degeneration, followed by dissection, aortitis, and sinus of Valsalva aneurysm.
Gross Findings, Heart
Aortic insufficiency results in volume overload and cardiomegaly with left ventricular dilatation and concentric hypertrophy (see Chapter 143) (Fig. 173.1).
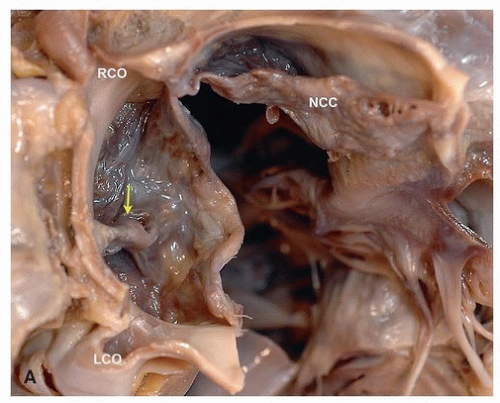 FIGURE 173.1 ▲ Aortic insufficiency with left ventricular dilatation, autopsy heart. A. The valve is opened with a cut at the commissure between the noncoronary and left side of the conjoint cusp and viewed from above. The arrow points to the raphe. RCO, right coronary ostium; NCC, noncoronary cusp; LCO, left coronary ostium. The deceased died suddenly and unexpectedly after refusing medical care for cough and shortness of breath. |
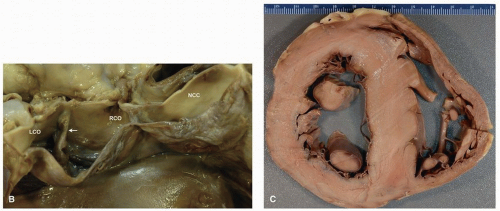 FIGURE 173.1 (Continued) ▲ B. Viewed from the side is the raphe. C. A short-axis section through the heart shows marked left ventricular dilatation. |
Aortic Insufficiency with Bicuspid Aortic Valve
Patients with bicuspid aortic valves develop valvular insufficiency at lower rate than that of stenosis, by about a factor of five.2,3 The mean age at valve surgery is in the early 50s for insufficiency, which is about 10 years younger than the typical age for severely symptomatic bicuspid aortic valve stenosis.2,4 Men are affected 7 to 17 times frequently than women, a higher differential than bicuspid aortic stenosis.2,3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


