Fig. 14.1
Hemorrhagic shock related to a retroperitoneal hematoma 2 weeks after pelvic surgery, with a discharge right nephrostomy to treat an iatrogenic lesion of the right ureter, while the patient was treated with low-molecular-weight heparin at curative dose because of a postoperative deep venous thrombosis of the lower limbs. (a) Non-enhanced CT scan: heterogeneous hypertrophy of the right lumbar psoas: hematoma, associated with an adjacent dense and heterogeneous wall hematoma. (b, c) Enhanced CT: several foci of blush in the lumbar wall hematoma. (d) CT scans few centimeters below: the hematoma involves the abdominal wall, the psoas, and iliac muscles. (e, f) Two selective lumbar arterial injections: the blush is found in the territory of the fourth right lumbar artery (arrow), leading to a hyperselective microcatheterization (f), before exclusion by microparticles and gelfoam
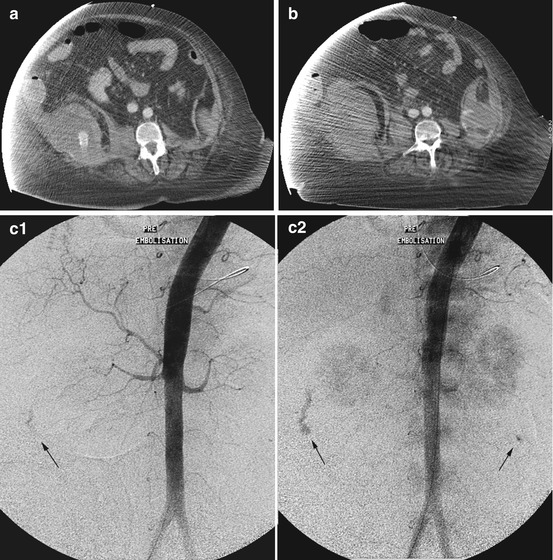
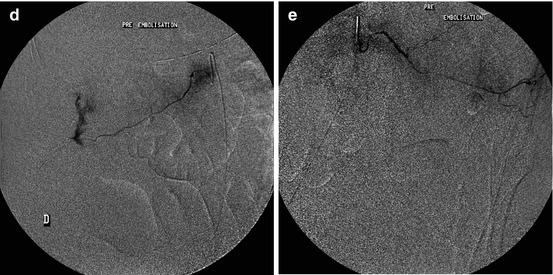
Fig. 14.2




Hemorrhagic shock in an obese patient treated by coumarin because of a rhythmic cardiopathy, in a status of DIC and multiple organ failure. (a) CT: right lumbar parietal hematoma, with important blush. (b) A few centimeters below: less important left lumbar parietal hematoma but also with important blush. (c1 and c2) Aortography: splanchnic generalized vasoconstriction, massive extravasation in the right lumbar wall, and blush in the left lumbar wall (arrows). (d) Selective catheterization of the third right lumbar artery supplying the extravasation: exclusion using microparticles. (e) Selective catheterization of the fourth left lumbar artery: hypervascularization of the psoas but also of the lumbar wall. The catheterization was very difficult because of an extreme fragility of the vascular wall, leading to an exclusion by coils
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
