Antiplatelet therapy in general should not be stopped prior to an intervention and all patients should be heparanised (e.g. 5000u i.v. bolus) during the procedure to prevent acute thrombosis. The risks are similar to catheter-directed angiography but with higher risk of acute thrombosis, dissection, haemorrhage and restenosis.
Interventions
Angioplasty and subintimal angioplasty.
Stent insertion (usually in conjunction with prior angioplasty).
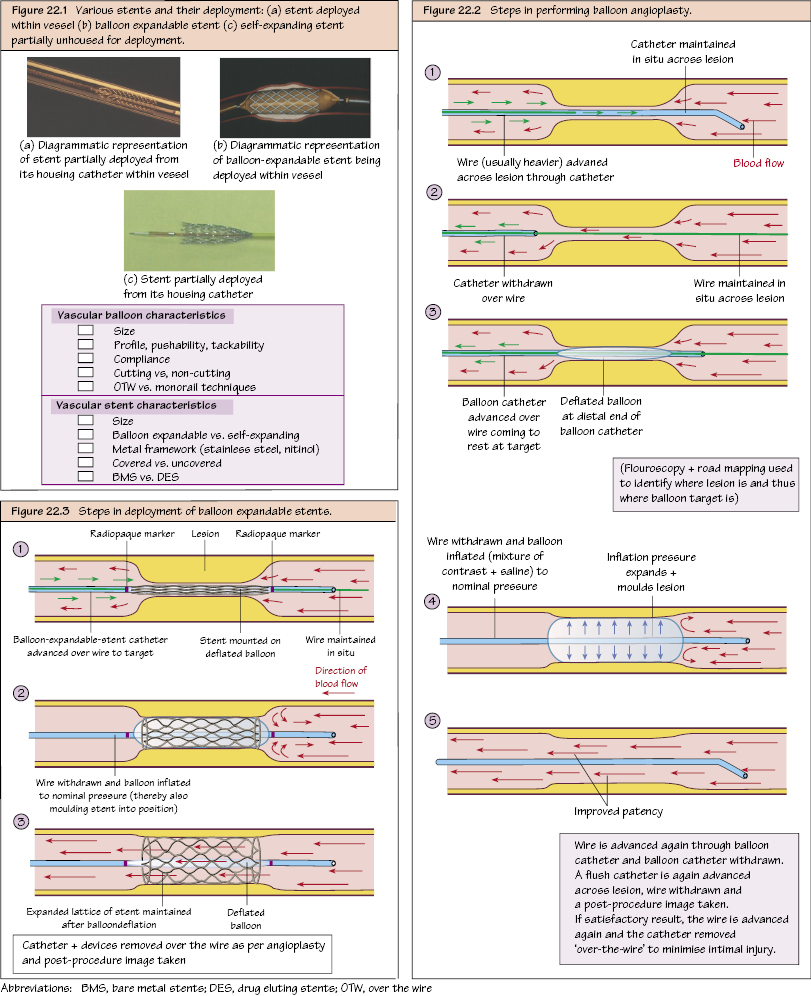
Balloon Angioplasty
A vascular balloon is inflated inside the stenosis and the pressure physically dilates and moulds the plaque against the vessel wall thereby opening up the flow. This can be performed as a therapeutic measure alone or prior to stent insertion.
The balloon is inflated to a pre-determined pressure using a hand-held pressure device (with manometer) and held for 30–60 seconds (repeated as necessary) followed by a check angiogram.
Dilute contrast (25–50%) is used so that the balloon can be visualised under fluoroscopy, but pure contrast has a high viscosity requiring higher pressures to inflate and is slower to deflate.
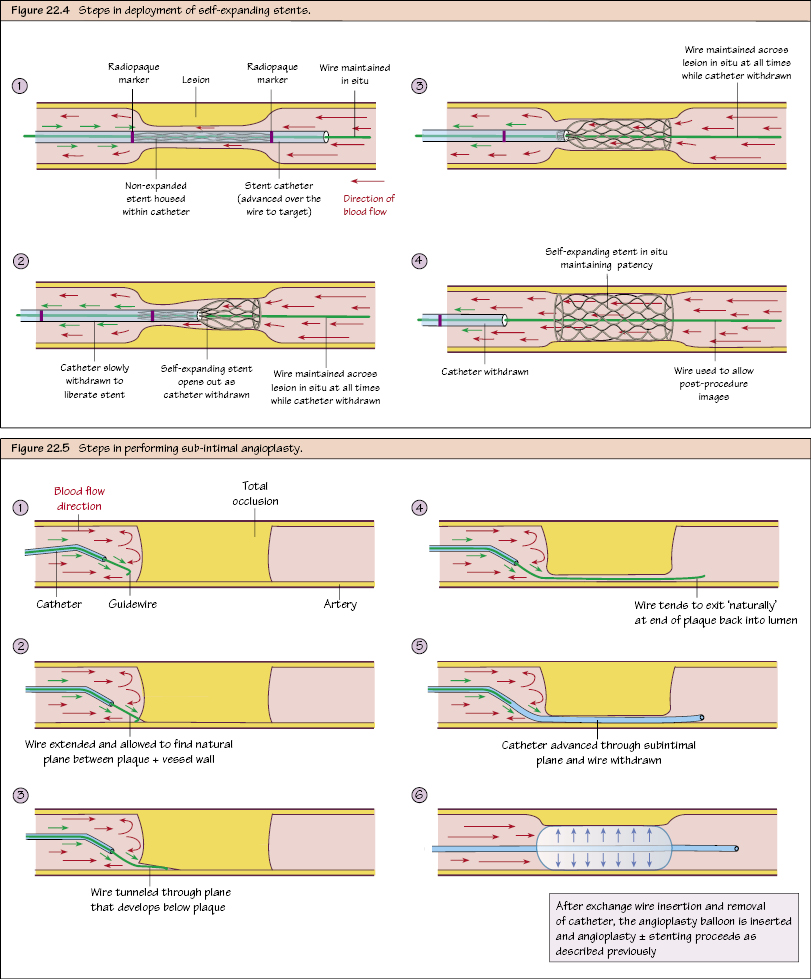
Sub-intimal angioplasty may be necessary in small vessels or where the stenosis cannot be crossed by the guidewire. Instead, the guidewire is allowed to find its own plane between the plaque and vessel wall, and to develop its own track after which it (usually) re-enters the lumen distal to the lesion. Angioplasty (±stenting) is then performed. There is a higher risk of rupture and pseudoaneurysm formation with this technique and patency rates are lower.
Angioplasty is considered a technical success when ≤30% residual stenosis remains immediately after the intervention compared with the pre-angioplasty images. However, it is the flow below the lesion that is more important for a good functional outcome.
Vascular Balloon Characteristics
Balloons are chosen according to size, compliance, deployment method
Only gold members can continue reading. Log In or Register to continue