All previous imaging and history should be reviewed to identify the target vessel(s) for imaging as well as the access vessel.
Identify any potential problems, especially renal failure, allergies and coagulopathy, and prepare appropriately.
In general, antiplatelet agents do not need to be stopped.
All devices for use should be pre-flushed with heparinised saline to remove any debris or air bubbles and to ensure patency.
Risks of procedure include allergic reactions, haematoma, bleeding, pseudoaneurysm, dissection and limb or organ ischaemia.
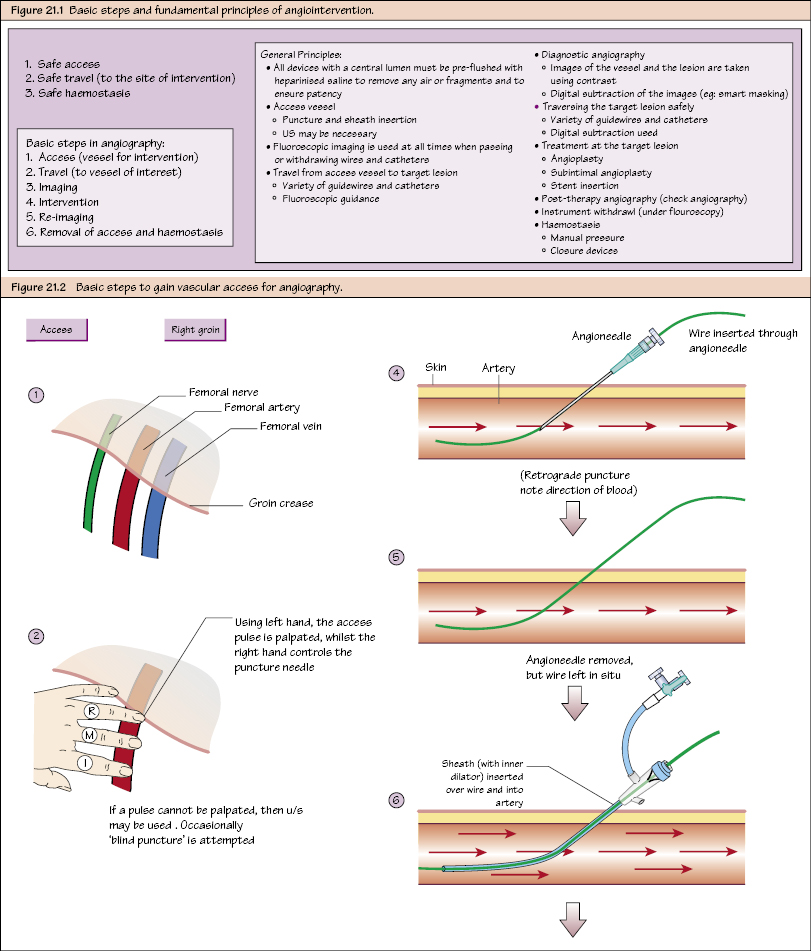
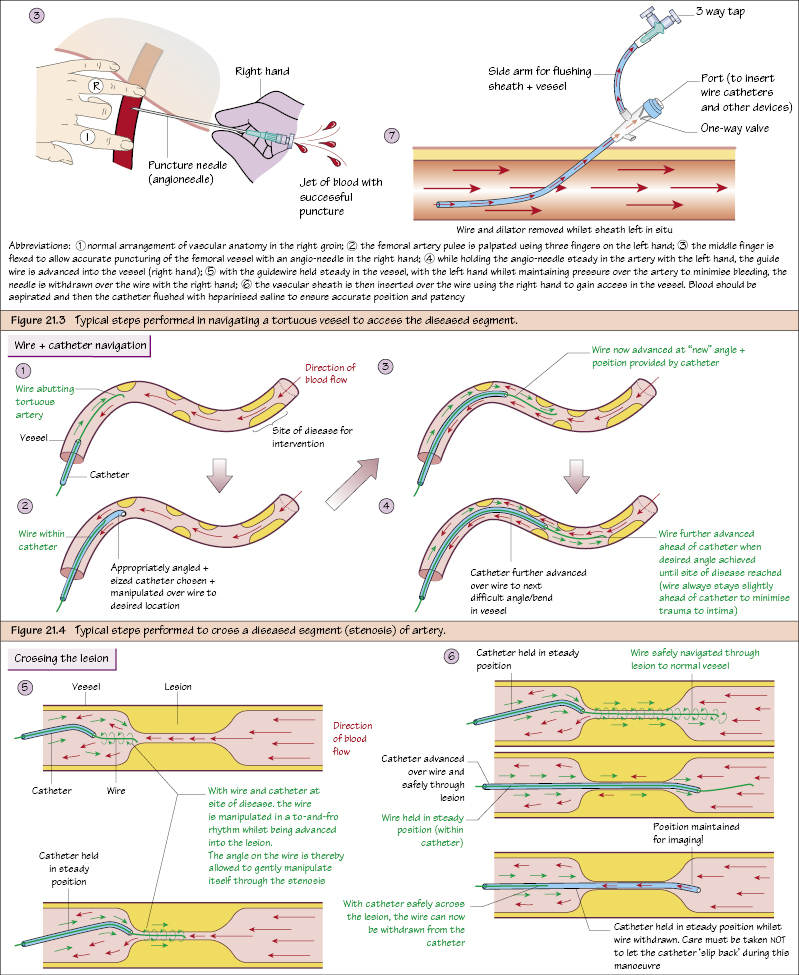
Access and Sheath Insertion
The access vessel is chosen (typically CFA) and manually palpated. (U/S is useful to locate an ideal puncture site if impalpable.)
A small skin incision is created and the access vessel is punctured using a wide-bore angiography needle (use a soft part of the vessel).
The puncture is typically retrograde (upwards against the flow of blood) but may also be antegrade (downwards in the direction of flow). Successful puncture is associated with pulsatile backflow of blood from the needle. Take care not to puncture the back wall or too high on the vessel (difficult to compress). Lower limb access is typically via retrograde puncturing of the contralateral limb.
After successful puncture, a short semi-stiff wire (0.035 inch) is inserted through the needle into the vessel and the angio-needle removed taking care to keep the wire in situ.
An appropriately sized, pre-flushed sheath (plastic access device) is then threaded over the wire and left in situ
Only gold members can continue reading. Log In or Register to continue