The standard resting 12-lead ECG records the heart rhythm for no more than 30s and is therefore not suitable for detecting intermittent disturbances in heart rhythm. Ambulatory ECG monitoring is an invaluable diagnostic tool. The ECG can be continuously or intermittently recorded for long periods.
Continuous ECG recording
The ECG can be continuously recorded, usually for 24–120 hours, using a portable battery-operated recorder that is usually worn around the neck or waist. The ECG is recorded in digital form in a solid state recording system. If appropriate, the patient can be fully ambulant, carrying out his or her normal day-to-day activities.
The ECG is recorded by means of adhesive electrodes applied to areas of thoroughly cleaned skin. Usually one electrode is placed over the upper sternum and the other electrode over the V5 chest lead position. As an alternative, a modified V1 lead can be obtained by placing one electrode over the V1 chest lead position and the other electrode beneath the lateral part of the left clavicle.
Figure 22.1 The artefact in the upper trace might have been misinterpreted as ventricular fibrillation had not the lower trace been recorded simultaneously.
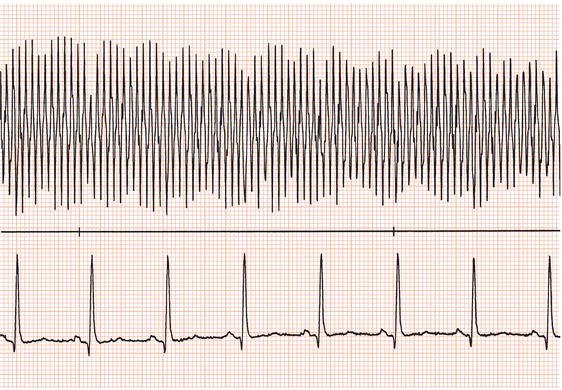
Figure 22.2 The lower trace suggests AV block but the simultaneous upper trace clearly shows that the small complexes in the lower trace are not P waves.

Most systems allow simultaneous recording of two or more leads. This increases diagnostic accuracy and aids in the detection of artefacts, which are unlikely to appear on both leads at the same time (Figure 22.1). Furthermore, sometimes one lead does not reveal important diagnostic information while the other does (Figure 22.2).
The recording is analysed by replaying it at 60–100 times real-time. Playback systems have facilities for printing out selected portions of the recording on ECG paper at standard speed. Most recording systems can automatically detect bradycardias, tachycardias and ectopic beats, though in practice an operator has to supervise the analysis.
Artefacts
Several technical problems during ambulatory electrocardiography can result in what appear to be arrhythmias to the unwary.
Not infrequently, a lead will become disconnected during a recording: because no activity is being recorded the ECG will appear as a straight line and mimic sinus arrest. Furthermore, sometimes an electrical connection can intermittently fail, resulting in repeated episodes of apparent sinus arrest. However, if a lead becomes disconnected it may do so at any point in the cardiac cycle, and it is unlikely the onset of ‘asystole’ will arise after the ventricular T wave as it would if sinus arrest were real. If the onset of sinus arrest occurs during the inscription of an atrial or ventricular complex, artefact can be assumed (Figure 22.3a).
Figure 22.3 (a) Artefact due to intermittent lead disconnection: apparent asystole can be seen to start during inscription of a T wave. (b) On close inspection narrow QRS complexes (indicated by letters N and A at the bottom of the trace) can be seen walking through apparent ventricular arrhythmia.

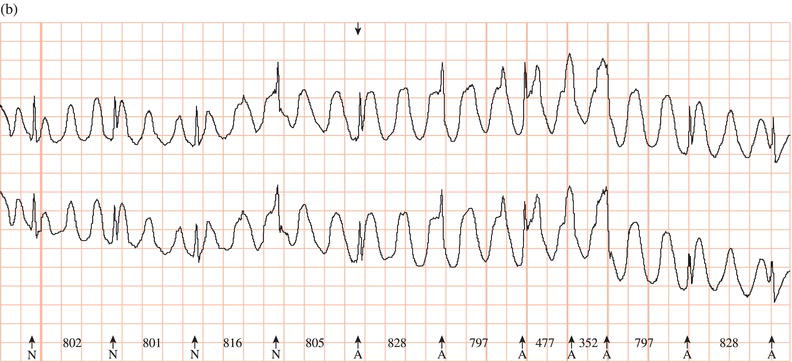
Occasionally, artefact can produce an apparent tachycardia, but close inspection will reveal that normal QRS complexes are ‘walking through’ the tachycardia (Figure 22.3b).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


