2 Advanced Echocardiography Approaches
3D Transesophageal Assessment of the Mitral Valve
Background
• Proper MV function depends on a balance between closing forces generated by the LV and tethering forces generated by the chordal attachments to the papillary muscles, which prevent the leaflets from prolapsing into the left atrium (LA) (Fig. 2-1).
• Each papillary muscle (PM) sends chordae to both leaflets. The posteromedial PM sends chordae to the posteromedial aspect of both leaflets, and the anterolateral PM sends chordae to the anterolateral aspect of both leaflets.
• During ventricular systole, the PMs contract to offset the loosening of the chordal forces that occurs with movement of the MV annulus toward the left ventricular (LV) apex in systole.
• The mitral annulus has a bimodal “saddle” shape, with high or superior points at the anterior and posterior parts of the annulus and the low or inferior points located at the medial and lateral parts of the annulus.
• Finite element modeling of the annulus has demonstrated that a bimodal shape is optimal to minimize stress on the MV during opening and closing.
• Mitral leaflets have inherent redundancy in order to have overlap of the leaflets at the coaptation line.
• This overlap region, often termed the “coaptation zone,” is felt to be important for the leaflets to properly “seal” the mitral orifice and prevent pathological mitral regurgitation (MR).
• Transmitral gradients are determined by flow across the MV, which in turn is influenced by the left atrial (LA) to LV pressure gradient.
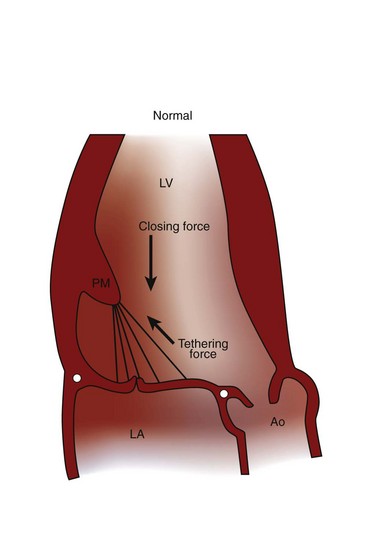
Figure 2-1 Mitral valve (MV) function results from a balance of closing forces and tethering forces.
Overview of the 3D Transesophageal Echocardiographic Approach
• Although accurate 3D reconstructions were obtained, this approach involved significant post-processing and careful respiratory and echocardiographic gating.
• 3D transthoracic echocardiography (TTE) provides standard and nonstandard imaging planes. It can be used as the only imaging modality but more often is used in a complementary role to 2D imaging.
• Although real-time 3D imaging represents a significant advance in echocardiographic technique, image resolution remains a limitation of 3D TTE.
• However, the recent introduction of 3D transesophageal echocardiography (TEE) has improved image resolution and is ideally suited to assess MV anatomy and function.
• The matrix array 3D TEE probe allows for several 3D imaging modes, each of which has advantages and limitations.
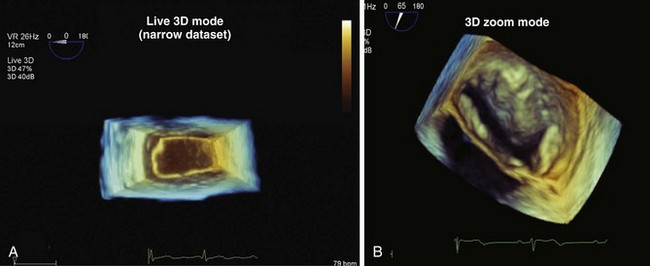
• Live 3D: This mode displays a real-time fixed-volume, 50 × 30 degree, pyramidal dataset (Fig. 2-2A). Simplicity is the major advantage of the live 3D mode. A 3D image is displayed in real time without need for optimization of the image alignment in the display field. The major disadvantage is that the fixed volume size of the live 3D mode may not be of adequate size to capture the structure or area of interest.
• 3D Zoom: This mode displays a truncated pyramidal dataset of variable size (see Fig. 2-2B). The advantage of this mode is that the 3D volume can be adjusted by the operator to include the entire area of interest (e.g., the MV). However, as the volume is set larger, the frame rate and thus image resolution decrease.
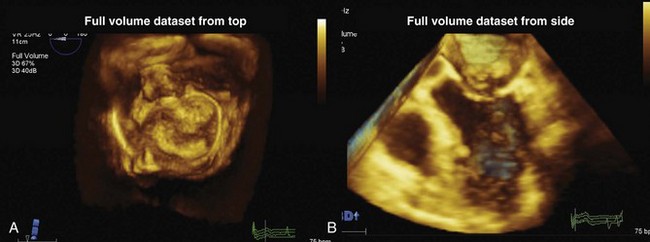
• Full-volume: This mode displays a 100 × 100 degree pyramidal dataset (Fig. 2-3). The MV should be aligned optimally in the middle of the image field using the biplane display, and, if possible, respiration should be suspended prior to full volume. Acquisition of a full volume dataset requires merging of smaller 3D pyramidal datasets obtained from 4–7 gated cardiac cycles (Fig. 2-4). The number of cycles can be preset. The greater the number of cycles, the higher the frame rate; however, the acquisition time is longer. The advantage of the full-volume mode is that it displays a large volume of data at a higher frame-rate than is possible with the 3D zoom mode. Because a full volume dataset is obtained by “stitching” together smaller pyramidal datasets, it is subject to “stitching artifacts” due to poor merging of the smaller pyramidal volumes caused by respiratory/transducer motion and/or arrhythmia (Fig. 2-5). Significant stitch artifacts will make the 3D datasets uninterpretable. Another disadvantage is that the dataset is not truly a “live” image.
• 3D Color Doppler: This mode displays a pyramidal volume of color Doppler data superimposed upon a volume of gray scale data (Fig. 2-6). Due to the low frame rate, 3D color Doppler is acquired by volume rendering. This gated reconstruction requires 7 to 14 cardiac cycles. The greater the number of cardiac cycles, the better the frame rate. However, the increase in cardiac cycles comes with a greater risk of a stitching artifact. Additional disadvantages include a significantly smaller pyramidal color volume compared with full volume imaging mode, which limits a comprehensive display of the complete color Doppler signals.




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
