Chapter 7 Adult congenital heart disease
Introduction
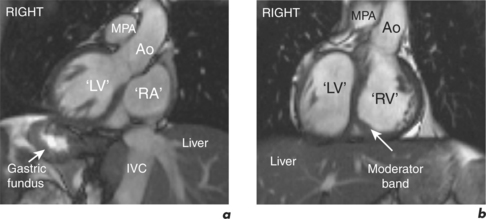
Congenital heart disease has an incidence of approximately 1% (Figure 7.1). Advances in medical and surgical management have resulted in a growing population of young adults who require continued care due to the predominantly palliative rather than curative nature of their interventions. CMR provides safe serial assessment of patients with adult congenital heart disease (ACHD).
CMR images and measurements complement those obtained using echocardiography, especially in postoperative patients. Accurate anatomical and functional information of complex cardiac pathology can be obtained in any plane. These factors make pre- and post-intervention CMR evaluation in ACHD invaluable.
CMR protocol
Other reporting requirements are highlighted following discussion of specific conditions.
Cardiac morphology and function
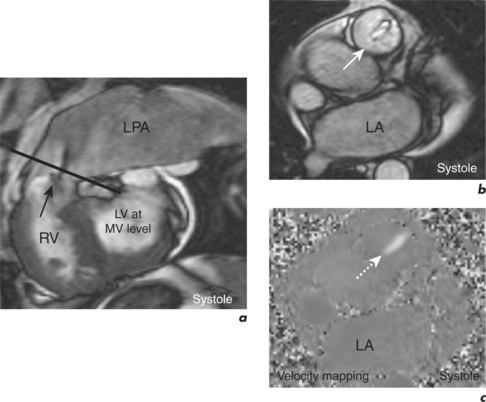
Subsequent cines are acquired in planes determined by the underlying diagnosis and provide higher resolution anatomical and functional information on parameters including biventricular size, function and mass. Assessment of the RV and pulmonary vasculature is of particular importance in ACHD along with extensive flow velocity mapping for measurement of peak velocities, regurgitant fractions and shunt performance (Figure 7.2). The Venc is set to account for low velocities in venous systems and higher velocities within shunts. Information from both the cines and velocity mapping is crucial for interpretation of the patterns of blood flow. Cine images also direct optimal positioning of velocity mapping sequences.
CMR in specific ACHD
Congenital heart disease is usually recognized in childhood and the most frequent use of CMR is in the assessment of patients with an established diagnosis.
Ventricular septal defect
VSDs are the most common congenital heart defects. They range from small haemodynamically insignificant and isolated lesions to large defects associated with multiple cardiac anomalies such as in TOF. CMR is complementary to echocardiography in the assessment of simple and complex VSDs. It allows multiplanar visualization of the spatial relationship of the defect to surrounding structures, can diagnose concurrent cardiac pathology and their functional sequelae, and quantify shunt size and effect on the RV and PAs. SE imaging en-face and parallel to the VSD provides anatomical information. SSFP cines show signal loss in the RV due to blood flow through the VSD and are useful in assessing the shape and dimensions of the defect (Figure 7.3). Shunt ratio can be calculated in two ways: firstly, comparison of pulmonary to systemic flow (Qp:Qs) obtained by velocity mapping CMR, and secondly, from the difference in ventricular SV obtained from the ventricular short-axis stack of cines (Figure 7.4).
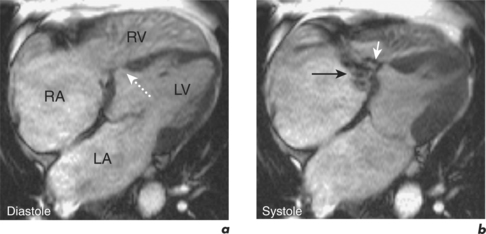
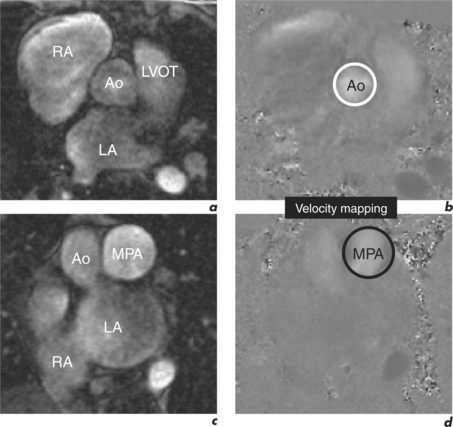
Figure 7.4 Calculation of Qp:Qs for the VSD case presented in Figure 7.3 using velocity mapping CMR.
Specific reporting features in the CMR assessment of VSD are therefore:



