We read the article by Lee et al in a recent issue of American Journal of Cardiology (May 2015) regarding the temporal influence of heart failure (HF) hospitalizations before implantable cardioverter defibrillator (ICD) or cardiac resynchronization therapy with defibrillator (CRT-D) on subsequent outcome in patients with mild HF with left bundle branch block and QRS prolongation, using data from the Multicenter Automatic Defibrillator Implantation Trial With Cardiac Resynchronization Therapy trial. The authors highlight the impact of a previous HF hospitalization ≤12 months in increasing risk for subsequent HF hospitalization or death compared with a previous HF hospitalization >12 months and no previous HF hospitalizations. Furthermore, the authors report evident clinical benefit of CRT-D over ICD in all patients regardless of time from last HF hospitalization. They logically conclude that a recent HF hospitalization should not be considered a disqualifying factor when selecting patients for CRT-D implantation. More importantly, they conclude that as a recent (<12 months) HF hospitalization identifies a higher risk group, these patients should receive CRT-D therapy if they meet the other standard criteria for this for this intervention.
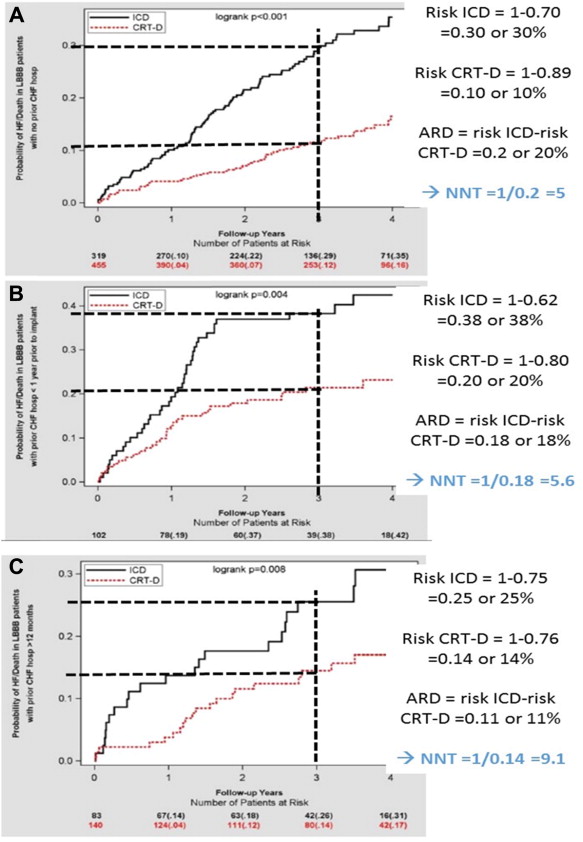
In this insightful manuscript, the investigators did not express the treatment effect of CRT-D over ICD according to the former hospitalization status on an absolute scale, that is, absolute rate or risk difference or corresponding number of patients needed to treat (NNT). Yet, readers can easily capture this practical and informative figure from published results. Analyzing on an absolute scale the survival curves provided in the article ( Figure 1 ), we may find that the absolute risk difference at 3 years is 11% (corresponding to an NNT = 9.1) in patients without previous HF hospitalization; 18% (NNT = 5.6) in those with recent HF hospitalization (<12 months); and 20% (NNT = 5) in those with without recent HF hospitalization (>12 months). From these data, we, indeed, observed that the absolute benefit from CRT-D is magnified in patients with recent HF hospitalization. The overall trend of higher absolute treatment effect on the basis of NNT within the groups is, to some extent, contrasting with the analysis based on hazard ratios provided in the report (hazard ratios being closer to one in patients with recent HF hospitalization than in those without previous HF hospitalization). Importantly, the reinterpretation we provided is a direct observation that a greater absolute effect is observed in patients with recent HF hospitalization and not a presumption based on higher baseline risk and similar treatment effect on a relative scale, as what was reported in the initial report.