CASE 9 Unprotected Left Main Coronary Intervention
Cardiac catheterization
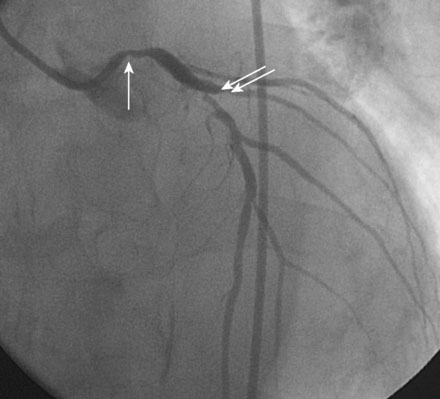
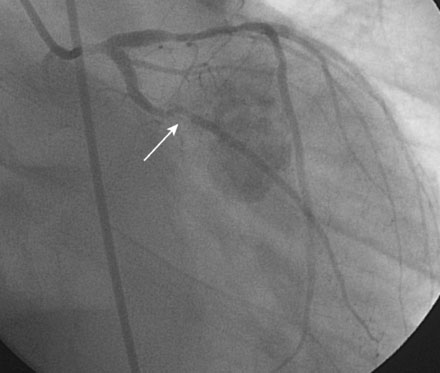
Obtaining arterial access proved challenging as his longstanding paraplegia resulted in substantial lower extremity atrophy and contracture at the hip. The femoral pulses were barely palpable; however, the right femoral artery was finally accessed successfully using ultrasound guidance, and angiography showed a small, diseased external iliac (Figure 9-1). The right coronary artery was without significant disease (Figure 9-2). Upon engagement of the left coronary artery, the operator observed pressure damping and ventricularization. The left main stem was severely diseased at the ostium (Figures 9-3, 9-4 and Videos 9-1, 9-2). In addition, there was significant obstructive disease noted in the proximal left anterior descending (LAD) and circumflex (LCX) arteries.


The operator inserted an 8 French sheath in the right femoral artery and procedural anticoagulation was achieved with bivalirudin; he had already been on clopidogrel therapy. An 8 French, left Judkins guide catheter was engaged and floppy-tipped guidewires passed into the LAD and LCX. The lesions in the LAD and LCX were treated successfully with balloon dilatation followed by placement of paclitaxel-eluting stents (Figure 9-5).

In order to protect the circumflex artery, the operator chose to use a modified “crush stent” technique to treat the left main stem lesion. Two stents were positioned in the left main/LAD and LCX: a 3.0 mm diameter by 20 mm long paclitaxel-eluting stent in the left main into the LAD, and a 3.0 mm diameter by 12 mm long paclitaxel-eluting stent in the circumflex (Figure 9-6). The left circumflex stent was deployed first (Figure 9-7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


