Chest radiograph at time of evaluation for thromboendarterectomy
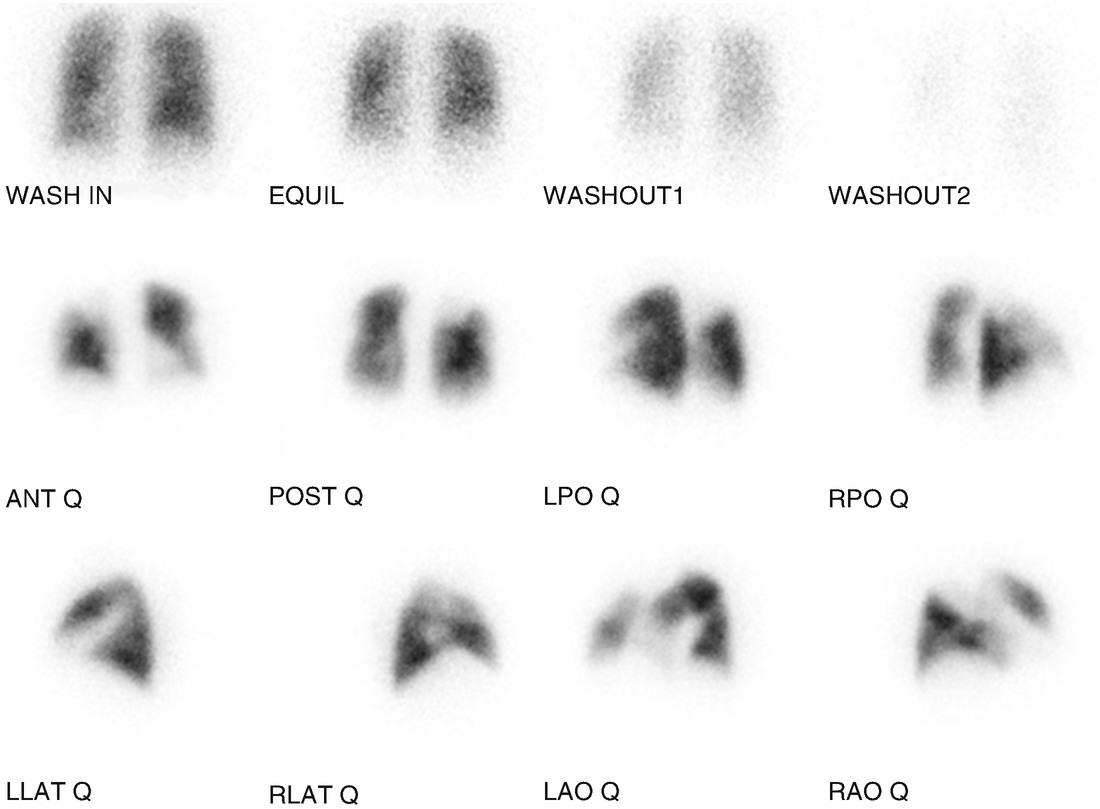
Lung scintigraphy demonstrating unmatched perfusion defects in both lungs
Results of the right heart catheterization showed pulmonary hemodynamics at rest of right atrial mean of 6 mmHg, PA pressure 31/13 mmHg (20 mean), PAOP 10 mmHg, thermodilution cardiac output of 7.2 L/min (cardiac index 3.17 L/min/m2) and calculated PVR 112 dyn s/cm5. Exertion of his upper extremities resulted in a PA pressure of 46/12 mmHg (28 mean), a pulmonary capillary wedge pressure of 12 mmHg, and a thermodilution cardiac output 13.6 L/min (cardiac index 5.99 L/min/m2); calculated PVR was 94 dyn s/cm5.
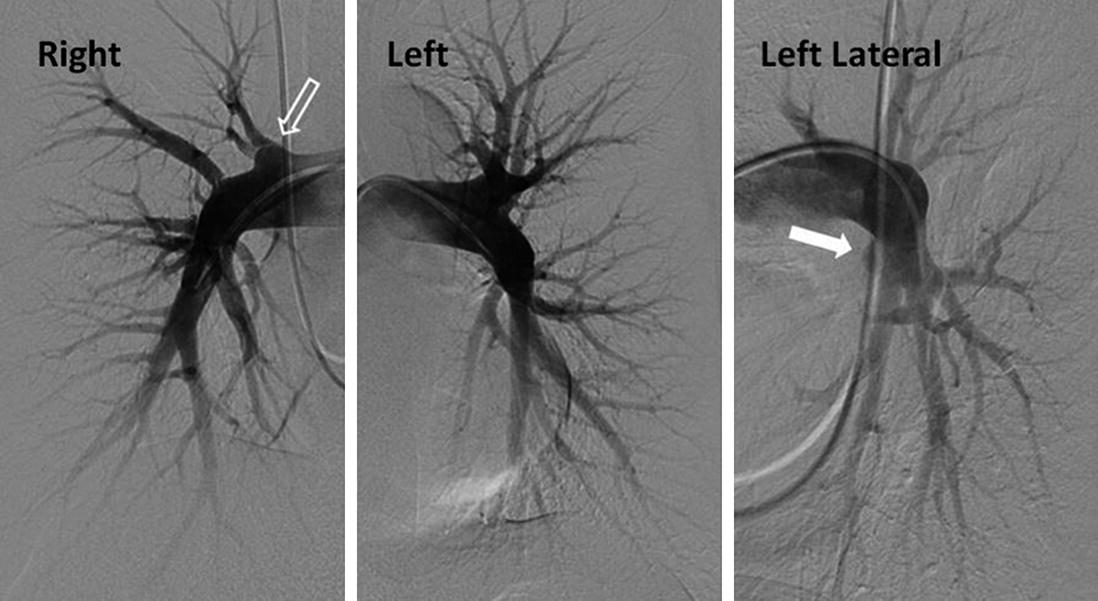
Digital subtraction pulmonary arteriogram: “pouch defect” proximal right upper lobe (open arrow), and occluded lingula (closed arrow)
Though there was radiographic evidence for operable chronic thromboembolic disease, in the absence of significant exercise limitation and with essentially normal pulmonary hemodynamics at rest and during modest exertion, it was assessed that the risk of a surgical thromboendarterectomy was unwarranted and unlikely to result in a noticeable clinical benefit. However, to provide a more complete physiologic evaluation at higher levels of exercise, a cardiopulmonary exercise test (CPET) was requested.
This was a maximal exercise test.
The patient reached >100% of maximal predicted oxygen consumption, consistent with supra-normal aerobic exercise capacity.
Normal cardiac response to exercise, with no evidence of impairment of heart rate or stroke volume reserve.
There was no evidence of a ventilatory limitation.
There was modest oxygen desaturation (nadir 92%), however, the SpO2 did not fall below 95% until a VO2 was twofold the value at the onset of anaerobic threshold and >100% of the maximal predicted VO2.
The absence of significant ventilatory inefficiency at peak workload as well as the absolute fall in the VE/VCO2 throughout exercise is consistent with relatively normal pulmonary vascular recruitment with exertion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


