CASE 60 Chronic Occlusion of a Superficial Femoral Artery
Case presentation
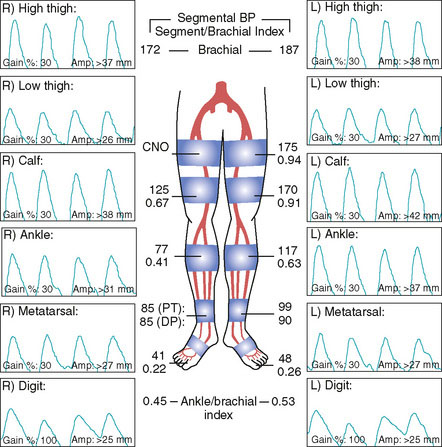
A 76-year-old woman developed worsening leg claudication, progressing nearly to rest pain. She had numerous atherosclerotic risk factors including diabetes, hypertension, hyperlipidemia, and prior tobacco abuse, and had an extensive atherosclerosis history including coronary artery disease, renal artery stenosis, cerebrovascular disease, and peripheral arterial disease. Six months prior to her current presentation, she underwent lower extremity angiography and was found to have bilateral iliac artery lesions along with disease in the superficial femoral arteries. At that point, her physician decided to first treat the inflow disease with stents and then reevaluate the patient’s symptoms. Following the bilateral iliac stenting procedure, she continued to have lifestyle-limiting claudication and her right leg symptoms progressed to occasional nocturnal rest pain. The noninvasive studies obtained after iliac stenting showed severe arterial insufficiency in both legs at the level of the thigh (Figure 60-1) consistent with the disease in the superficial femoral artery (SFA). Her physician recommended repeat angiography and possible SFA intervention.
Angiography
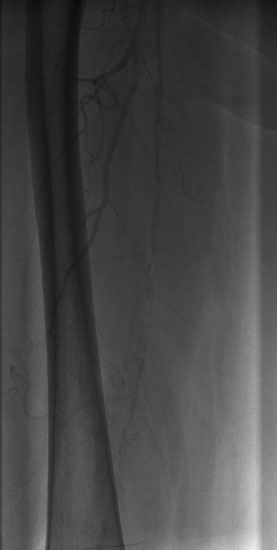
Arterial access was obtained in the left common femoral artery and a 4 French Omniflush catheter was used to perform angiography. Aortography confirmed wide patency of the common iliac stents (Figure 60-2). Selective right femoral angiography and runoff was performed by passing a hydrophilic glide wire over the bifurcation using the Omniflush catheter and then exchanging for a 4 French RIM catheter. Angiography found a mild stenosis in the common femoral artery, followed by a diffusely diseased segment of the proximal SFA of moderate stenosis and then a long segment of total occlusion (Figure 60-3). There was reconstitution of the distal SFA above the adductor canal via collaterals from the profunda femoris (Figures 60-4 through 60-6). Below the knee, the anterior tibial was occluded; however,two-vessel runoff was present to the foot via the posterior tibial and peroneal arteries. Based on the patient’s profound symptoms, her anatomy, and her comorbid conditions, it was decided to proceed with an intervention to the right SFA.
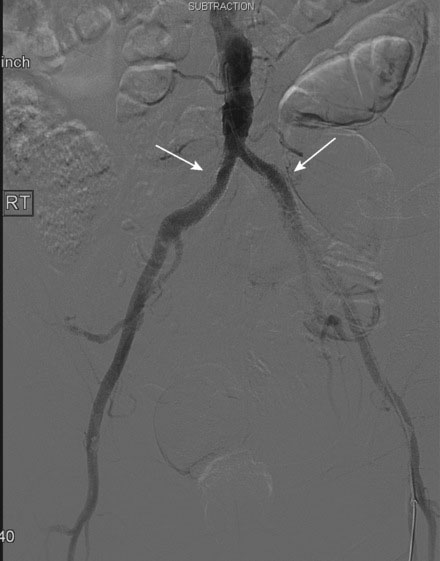

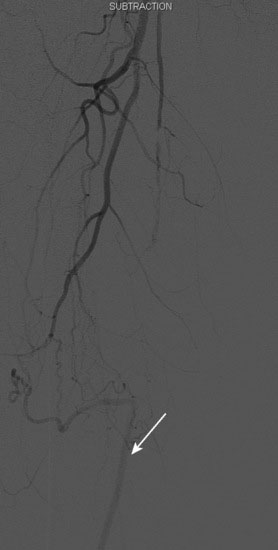
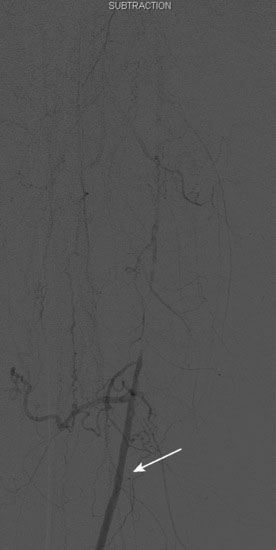
FIGURE 60-4 A long occlusion of the mid-SFA is present and reconstitutes at the popliteal artery (arrow).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


