CASE 58 Iliac Artery Disease
Case presentation
A 64-year-old woman with a history of hypertension, hyperlipidemia, and tobacco use noted progressive bilateral calf discomfort during activity. These symptoms slowly progressed, and ultimately they became so severe that she stopped participating in tennis, her favorite activity. She discussed these symptoms with her primary care physician. Her physician interpreted these symptoms as claudication and ordered noninvasive vascular testing. Her resting ankle brachial index (ABI) was 0.75 on the right and 0.58 on the left (Figure 58-1). After exercise, her right ABI dropped to 0.60 and her left ABI dropped to 0.21. In addition, exercise caused significant bilateral calf pain, with the left side hurting more than the right. She was subsequently referred for angiography.

Angiography
Abdominal angiography found normal renal arteries and distal aorta. Angiography of the pelvic vessels demonstrated a severe stenosis of the left external iliac artery (Figures 58-2, 58-3). Initially, there did not appear to be appreciable disease in the right iliac system to account for the findings on the noninvasive study; however, there was significant vessel overlap. The femoral and runoff vessels appeared normal bilaterally.


The left external iliac lesion was felt to be consistent with her noninvasive studies and likely accounted for her symptoms. The etiology of her right leg findings was not apparent on the initial angiograms. The operator decided to proceed with intervention of the left external iliac. Arterial access had initially been obtained in the right common femoral artery for the diagnostic angiograms. A long, 6 French Ansel 2 sheath was taken up and over the aortoiliac bifurcation and positioned proximal to the left external iliac lesion. A bolus of unfractionated heparin was administered intravenously to achieve a therapeutic activated clotting time of greater than 250 seconds. The operator positioned an 0.018 inch guidewire distally (Figure 58-4) and dilated the stenosis with a 5 mm diameter by 40 mm long balloon (Figure 58-5). Following balloon angioplasty, substantial residual narrowing remained due to elastic recoil. The operator then deployed a 7 mm diameter by 40 mm long self-expanding nitinol stent and postdilated the stent with the 5 mm diameter by 40 mm long balloon. The post-stent angiogram revealed an excellent result (Figure 58-6) and angiography of the distal runoff showed no distal emboli.

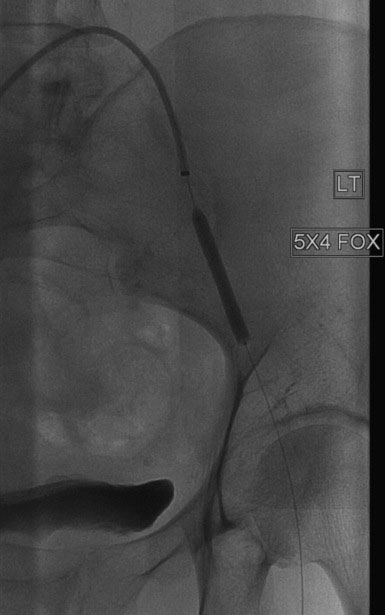

FIGURE 58-6 Angiographic appearance of the left external iliac artery following angioplasty and stenting.
Following the procedure on the left external iliac artery, the operator withdrew the long sheath over a 0.035 inch wire. Pressure monitoring during the pullback uncovered a 60 mmHg pressure gradient between the distal aorta and the distal right external iliac. Another angiogram was performed, which found a stenosis just proximal to the inguinal ligament (Figure 58-7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


