CASE 5 Nondilatable Lesion
Cardiac catheterization
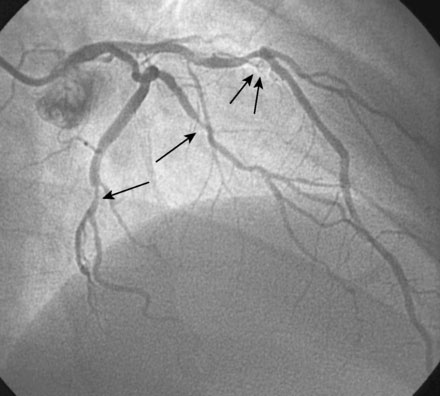
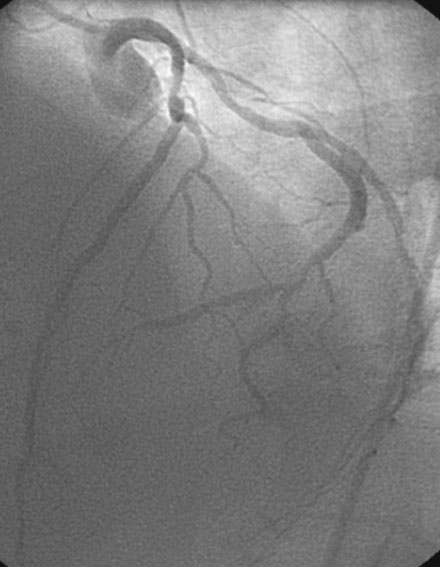
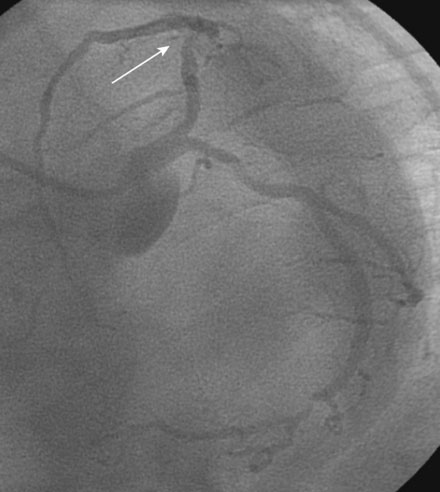
Ventriculography revealed normal left ventricular function. Coronary angiographic findings included a codominant circulation, with a diffusely diseased but small right coronary artery (Figure 5-1) and moderate distal disease in the left circumflex and obtuse marginal branches (Figures 5-2, 5-3). The proximal segment of the left anterior descending artery contained moderate disease (Figure 5-2 and Video 5-1) that in some views appeared nonobstructive (Figures 5-2, 5-3) but in other views appeared more concerning (Figure 5-4 and Video 5-2). Much of the disease present on this study appeared similar to the appearance on angiography 4 years earlier, leaving the operator at a loss for the dramatic change in symptoms.

The concerning symptoms, along with an ambiguous lesion in the proximal left anterior descending artery, prompted the operator to measure fractional flow reserve of this vessel (Figure 5-5). After a 6 French guide catheter was inserted, a pressure wire was advanced past the lesion and hyperemia induced with 100 μg of intracoronary adenosine; fractional flow reserve measured 0.69. Thus, the angiographically-moderate disease represented a flow-limiting lesion, and the operator decided to treat the lesion percutaneously. Following the administration of intravenous heparin and eptifibatide, the procedure began with balloon predilatation, using a 2.5 mm by 20 mm long compliant balloon. At nominal inflation pressure, a significant waist remained in the compliant balloon (Figure 5-6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


