History
In March 2012 this 68-year-old male patient sought treatment for chest pain. Non–ST segment elevation myocardial infarction (NSTEMI) was diagnosed, and, on catheterization, the patient was found to have severe three-vessel disease. This was unsuitable for percutaneous coronary intervention. He was therefore treated with bypass grafting and mitral valve repair.
The patient also had multiple myeloma (immunoglobulin G kappa), which was being treated with bortezimib and decadron; recurrent anemia resulting from myeloma and chemotherapy and requiring periodic blood transfusions; and thrombocytopenia. He was recommended to have platelet transfusions whenever his platelet concentration dropped below 20,000/µL or signs of bleeding occurred.
He had been previously diagnosed with mixed nonischemic and ischemic cardiomyopathy. He had a history of adriamycin exposure and thoracic radiation for myeloma. Magnetic resonance imaging 3 months previously revealed a severely dilated left ventricle (left ventricular ejection fraction [LVEF], 28%) with an akinetic inferior wall and left ventricular scar area of 9%. There was no evidence of infiltrative disease, for example, amyloidosis.
The patient had previously experienced frequent premature ventricular contractions, possibly contributing to left ventricular dysfunction. Their origin was the inferior scar margin, and they had been successfully ablated 3 months previously (December 2011). Programmed electrical stimulation at that time induced a sustained monomorphic ventricular tachycardia. In view of this, and baseline prolonged QRS duration with a left bundle branch block configuration, he received a cardiac resynchronization therapy defibrillator (CRT-D) implant (February 2012) with automatic remote monitoring capability. The implant was complicated by a significant anterior chest wall hematoma, but did not require evacuation. He had no prior history of atrial fibrillation.
The patient’s other significant comorbidities were chronic renal dysfunction, with a creatinine value normally approximately 2.0, and carotid artery disease, for which he had undergone left carotid endarterectomy in 2009.
Physical Examination
Thirty-six hours after cardiac surgery, the patient developed atrial fibrillation with a rapid ventricular response.
Laboratory Data
Postoperative Echocardiogram
On the echocardiogram a moderate pericardial effusion was seen adjacent to the right ventricle and right atrium measuring 2.3 cm and a small circumferential pericardial effusion adjacent to the left ventricle. Pleural effusions were noted bilaterally. The LVEF was 15 ±5%. The mitral valve ring had moderate (2+) mitral valve regurgitation.
Comments
An attempt was made to restore normal rhythm. Unusually, this case of postoperative atrial fibrillation was resistant to amiodarone therapy and electrical cardioversion. Sinus rhythm could not be maintained for even a few minutes.
Ideally, this patient should have been placed on anticoagulation therapy. However, this would have risked expansion of postoperative pericardial and pleural effusions in the setting of thrombocytopenia and predilection for occult bleeding. In view of this hematologic disorder, anemia, and general postoperative debilitation risking falls (requiring wheelchair), the risk to benefit balance favored postponing anticoagulation. This strategy nevertheless risked both thromboembolism and heart failure precipitated by reduction of CRT pacing level. However, because the patient had a device with remote monitoring, his condition could potentially be monitored closely without requirement for hospital visits. In particular, rate control could be optimized. The patient preferred this approach. He was discharged to a rehabilitation facility.
Follow-Up
Postoperative 2 Weeks
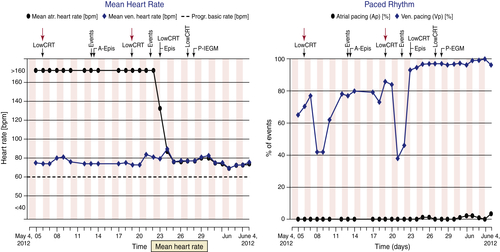
The patient was readmitted with decompensated systolic heart failure and continued atrial fibrillation, with ventricular rates exceeding 110 bpm (CRT pacing level <60%). He underwent thoracentesis. He was placed on diuretic therapy, and his heart failure medications were slowly optimized. This was a difficult balance in view of his systolic blood pressure of approximately 100 mm Hg. A sternal wound infection was discovered and treated with antibiotics. Tremor related to amiodarone exposure was noted.
Postoperative 4 Weeks
The patient was admitted with a chest infection, which was treated with antibiotics. He was anemic (hemoglobin 8.8 mg/dL and hematocrit 26%) and received transfusion.
Postoperative 6 Weeks
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


