CASE 48 Alcohol Septal Ablation for Hypertrophic Obstructive Cardiomyopathy
Cardiac catheterization
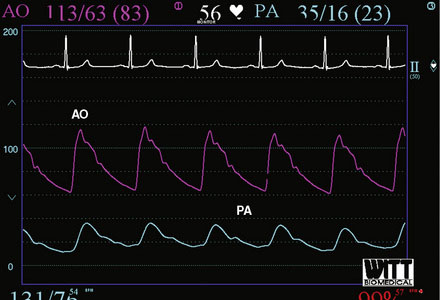
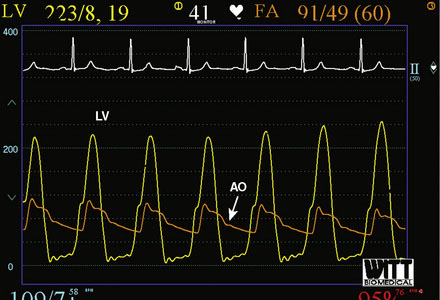
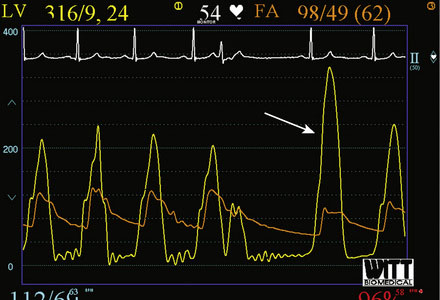
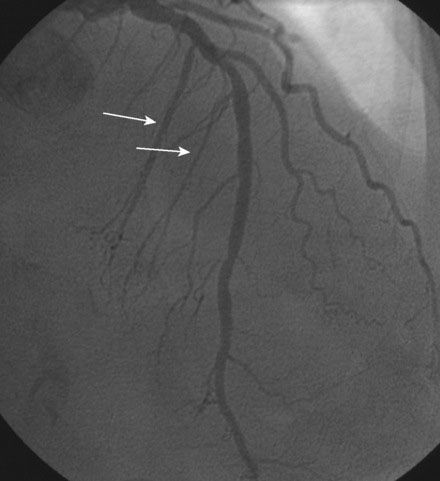
Right heart catheterization revealed a mean right atrial pressure of 4 mmHg, a pulmonary artery pressure of 34/14 with a mean of 21 mmHg, and a mean pulmonary capillary wedge pressure of 13 mmHg. The aortic pressure waveform exhibited the characteristic “spike and dome” morphology seen in hypertrophic obstructive cardiomyopathy (Figure 48-1). A multipurpose catheter with an end-hole and two side-holes at the tip was positioned in the left ventricular cavity. Simultaneous recording of left ventricular and femoral arterial pressure revealed a systolic gradient in excess of 100 mmHg at baseline; with provocation using a post-premature ventricular contraction the gradient exceeded 200 mmHg (Figures 48-2, 48-3). A slow pull-back of the catheter recorded no pressure gradient across the aortic valve (Figure 48-4). Left coronary angiography demonstrated several septal perforators appropriate for alcohol septal ablation (Figure 48-5 and Video 48-1).

To perform the alcohol septal ablation procedure, the operator first positioned a temporary pacemaker into the right ventricular apex and tested the threshold to ensure capture. An angioplasty guide catheter was engaged into the left coronary ostium and 50 U/kg of unfractionated heparin were administered. A floppy-tipped, 0.014 inch guidewire was advanced into the larger of the first septal branches and a 2.0 mm diameter by 8 mm long over-the-wire balloon catheter was advanced over the wire into the proximal segment of the first septal perforator. The operator inflated the balloon and injected iodinated contrast into the left coronary artery to prove that the balloon was occlusive, thus isolating the septal perforator from the left coronary circulation (Figure 48-6 and Video 48-2). The operator then removed the 0.014 inch wire from the balloon catheter and, with the balloon still inflated, injected iodinated contrast through the lumen of the balloon to show that there was no leakage of contrast from the septal artery to the left anterior descending artery (Figure 48-7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


