History
The patient was referred from another center for consideration of cardiac resynchronization therapy (CRT) for long-standing ischemic cardiomyopathy and progressive heart failure symptoms. At time of referral he described New York Heart Association (NYHA) class III symptoms despite optimal medical therapy.
The patient’s history included ischemic heart disease, first diagnosed at 40 years of age. At that time he also had exertional angina. A 12-lead electrocardiogram (ECG) showed left bundle branch morphology. Echocardiography and left ventriculography demonstrated impaired left ventricular function with a left ventricular ejection fraction of 40%. Coronary angiography demonstrated severe three-vessel coronary artery disease. He underwent coronary bypass grafting at 40 years of age, with left internal mammary grafting to the left anterior descending artery and saphenous vein grafts to the lateral circumflex and posterior descending arteries. He then remained asymptomatic until ventricular fibrillation arrest occurred while driving in a car race at 50 years of age. Coronary bypass grafts were intact, with no new native coronary lesions suitable for percutaneous intervention. Left ventricular function remained mildly impaired. Treatment with amiodarone was initiated, and he underwent implantation of an implantable cardioverter-defibrillator at that time. He had no further ventricular arrhythmias or device therapies delivered, but over the ensuing 8 years he developed progressive symptoms of heart failure accompanied by a decline in left ventricular systolic function. At the time of referral for CRT, he had no symptoms of ischemic heart disease and coronary angiography demonstrated patent grafts but diffuse native coronary disease.
Apart from hyperlipidemia, the patient had no history of other significant medical conditions.
Current Medications
The patient was taking spironolactone 25 mg daily, furosemide 120 mg daily, atorvastatin 20 mg daily, carvedilol 12.5 mg twice daily, enalapril 5 mg twice daily, amiodarone 200 mg daily, and enteric coated aspirin 100 mg daily.
Comments
Although the patient practiced good adherence to guideline–based heart failure medications, maximal doses of carvedilol and enalapril were not tolerated because of hypotension and azotemia. Occasional additional midday furosemide doses were self-administered by the patient according to an action plan based on weight and symptoms.
Current Symptoms
Physical Examination
Comments
Physical examination elicited signs consistent with left ventricular dysfunction and mild volume overload.
Laboratory Data
Comments
Hematologic investigations were within normal limits. Biochemical testing revealed mild renal dysfunction consistent with prerenal azotemia, with no evidence of intrinsic renal disease on subsequent testing.
Electrocardiogram
Findings
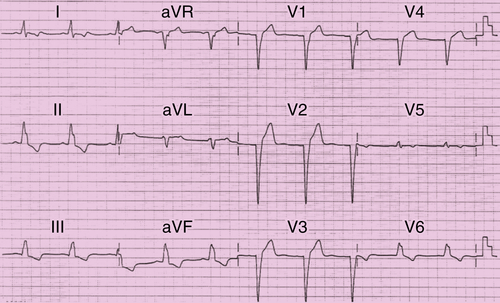
The ECG in Figure 46-1 shows a sinus rhythm of 60 bpm, left bundle branch block, and QRS duration of 190 ms.
Echocardiogram
Findings
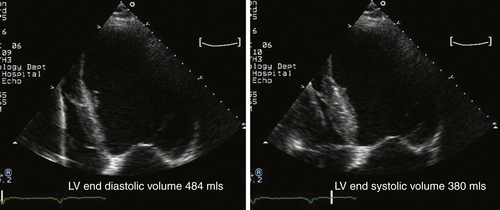
The echocardiogram showed severe left ventricular dilation with an end-diastolic volume of 484 mL, end-systolic volume of 380 mL, with severe global systolic dysfunction and calculated ejection fraction of 21% (Figure 46-2).
Comments
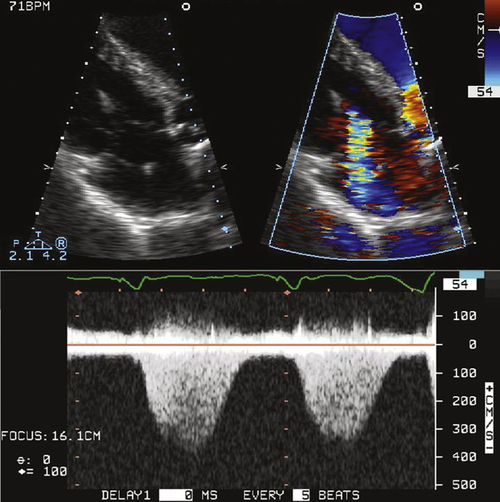
In addition to severe systolic dysfunction, evidence of mechanical dyssynchrony with a prolonged left ventricular preejection time of 190 ms was noted (Figure 46-3).
Findings
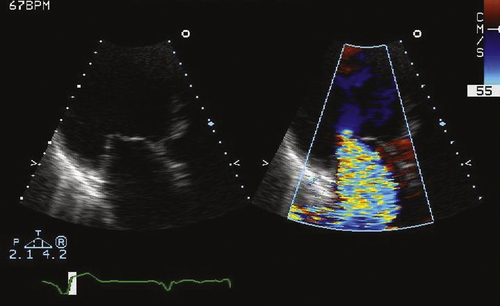
The echocardiogram also showed normal mitral valve leaflets, tenting of leaflets resulting from left ventricular dilation, severe functional mitral regurgitation, effective regurgitant orifice 0.5 cm2, and the regurgitant volume of 72 mL by the proximal isovelocity surface area method.
Comments
The findings on echocardiography were consistent with those of severe functional mitral regurgitation as a consequence of ischemic cardiomyopathy with severe ventricular dilation (Figure 46-4).
Findings
Moderately severe functional tricuspid regurgitation, with peak velocity of 3.8 ms, consistent with estimated right ventricular systolic pressure of 58 mm Hg above right atrial pressure.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


