CASE 45 Is Open-Heart Surgical Backup Necessary for PCI?
Cardiac catheterization
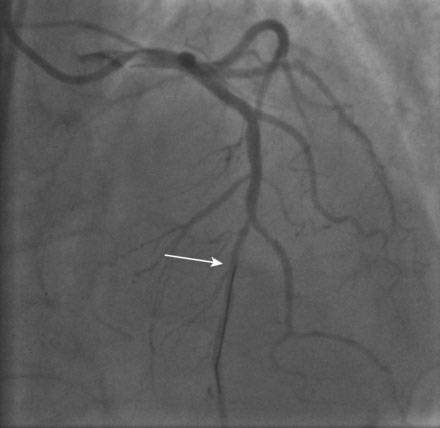
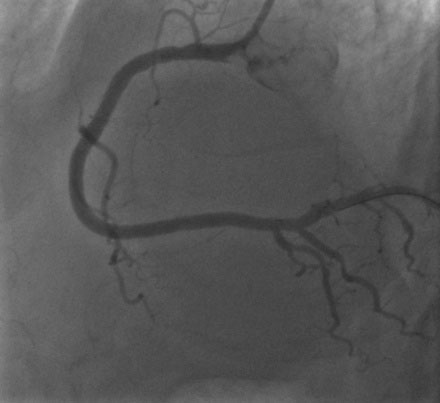
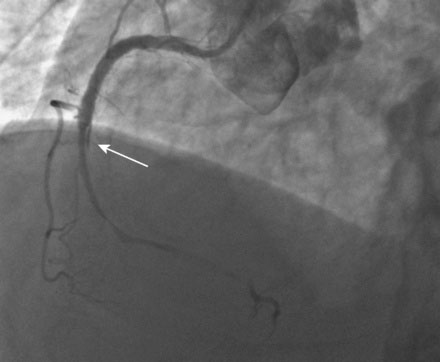
The patient stayed at the community hospital and the procedure was scheduled with an experienced interventional cardiologist (who performed more than 200 interventions each year), whose primary practice was at a large university hospital with surgical backup. Left ventricular function appeared normal with no wall motion abnormalities. The right coronary artery had a severe stenosis in the proximal segment; this lesion appeared hazy, but there was normal TIMI flow in the artery (Figure 45-1 and Video 45-1). The left coronary angiogram was notable for a normal appearing circumflex artery and a moderate lesion in the midsegment of the left anterior descending (LAD) artery (Figures 45-2, 45-3). To further assess the hemodynamic significance of the LAD stenosis, the operator measured fractional flow reserve (FFR); this calculated to 0.84 and was therefore deemed not significant.


Thus, the interventionalist proceeded with PCI and placed a 6 French right Judkins guide catheter in the right coronary artery after procedural anticoagulation was achieved with bivalirudin. The operator first dilated the lesion with a 3.0 mm diameter by 20 mm long compliant balloon and then placed a 4.0 mm diameter by 28 mm long drug-eluting stent. As the operator was satisfied with the angiographic result in several views (Figures 45-4, 45-5 and Videos 45-2, 45-3), intravascular ultrasound was not performed and the case was terminated. The patient felt well with no chest pain or discomfort. Hemostasis was easily accomplished with a vascular closure device.

The patient had been moved off the cardiac catheterization laboratory table and onto a stretcher awaiting transfer to his hospital bed when he reported chest pain, diaphoresis, and nausea. The monitor leads showed marked ST-segment elevation and sinus bradycardia. Fearing acute stent thrombosis, the patient was immediately returned to the cardiac catheterization laboratory and the physician quickly regained arterial access and imaged the right coronary artery. The right coronary was completely occluded distal to the stent and there appeared to be a linear dissection beyond the distal end of the stent that was not apparent on the post-PCI films (Figure 45-6). At this point, the patient had ongoing severe chest pain and bradycardia but maintained an adequate arterial pressure.
The operator administered atropine, unfractionated heparin, and eptifibatide, and attempted to open the artery. Gaining the true lumen proved extremely difficult, but finally the operator was able to insert floppy-tipped guidewires into both the posterior descending and the posterolateral branches (Figure 45-7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


