CASE 44 Crush Stent or Provisional Stenting for Bifurcation Lesion?
Case presentation
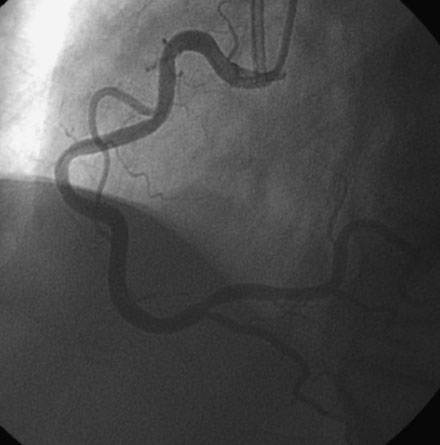
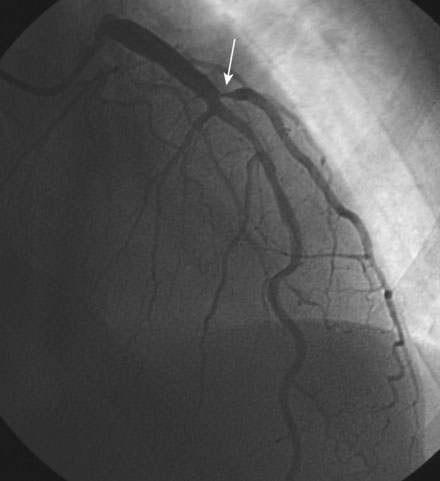
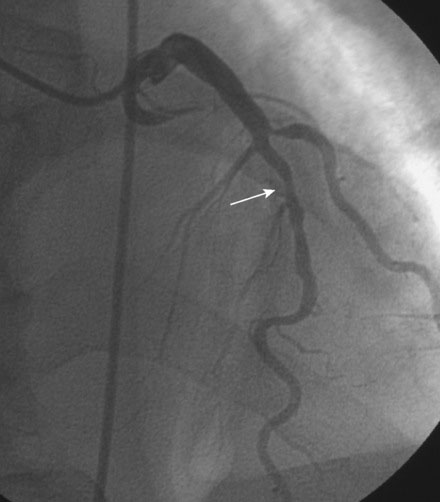
A 52-year-old man with end-stage renal disease, on dialysis for 5 months, developed ventricular tachycardia during vascular access surgery for dialysis. Past history was notable for longstanding and poorly controlled hypertension leading to end-stage kidney disease and a history of systolic heart failure, with an echocardiogram showing global left ventricular dysfunction and ejection fraction of 35% to 40%. He underwent cardiac catheterization 5 months earlier when he first presented with heart failure in the setting of renal failure, and was found to have a normal right coronary artery (Figure 44-1), a normal circumflex system, and moderate disease in the left anterior descending (LAD) artery just after the first septal perforator, but he also had a severe stenosis of the ostium of a large diagonal branch (Figures 44-2 through 44-4 and Video 44-1). Based on this evaluation, his heart failure and systolic dysfunction were thought to be secondary to the renal failure and hypertensive heart disease, with coexisting coronary artery disease. He was treated medically with lisinopril, metoprolol, aspirin, and amlodipine and did well until he developed sustained polymorphic ventricular tachycardia and chest pain during AV fistula graft placement for dialysis. This episode required resuscitation with cardioversion and intubation. Sinus rhythm was restored and subsequent electrocardiograms showed no acute changes but serial troponin I assays were elevated, consistent with a non-ST segment elevation myocardial infarction. He was loaded with clopidogrel and referred for repeat coronary angiography with the plan to treat the diagonal lesion previously observed.

Cardiac catheterization
The angiographic appearance of the coronary arteries had not changed since the prior catheterization. Because the diagonal artery was very large in caliber and vascular distribution and the disease involved the ostium of this vessel, and because there was also disease involving the left anterior descending artery at the bifurcation, the operator planned to use a “crush” stent technique to treat the complex disease of the LAD/diagonal bifurcation. After achieving therapeutic anticoagulation with unfractionated heparin, an 8 French, “C” left 4.5 guide catheter was engaged in the left coronary artery and floppy-tipped guidewires were placed in the diagonal and the LAD. A 3.5 mm diameter by 12 mm long paclitaxel-eluting stent was positioned in the diagonal at the ostium and a 3.5 mm diameter by 28 mm long paclitaxel-eluting stent was positioned in the LAD with the LAD stent spanning the ostium of the diagonal artery (Figure 44-5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


