CASE 43 Slow Reflow After PCI for Acute ST-Segment Elevation Myocardial Infarction
Cardiac catheterization
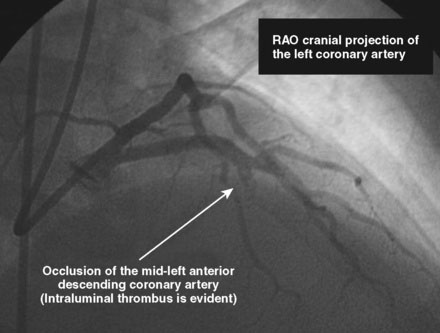
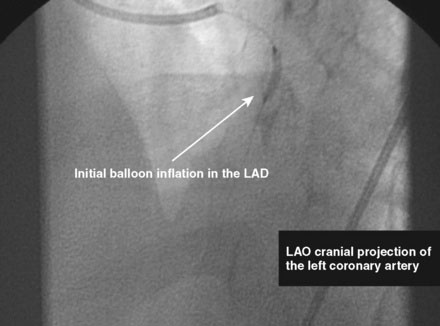
The initial coronary angiogram showed occlusion of the left anterior descending (LAD) coronary artery with the appearance of intraluminal thrombus (Figure 43-1 and Video 43-1). The circumflex and right coronary arteries were without significant obstruction. The operator decided to proceed with immediate PCI of the LAD. The ACT was adjusted with additional boluses of unfractionated heparin to maintain an ACT between 250 and 300 seconds, and eptifibatide was administered as adjunctive therapy (two intravenous boluses, each of 180 mcg/kg, and an infusion of 2.0 mcg/kg per minute continued for 14 hours). The left coronary artery was engaged with a JL4 guide, and the lesion was easily crossed with a 0.014 inch floppy-tipped guidewire. In this case, a thrombus extraction catheter was not used. The operator centered a 2.5 mm diameter by 15 mm long compliant balloon on the lesion and inflated it to 6 atmospheres of pressure (Figure 43-2). Following balloon angioplasty, there was a good angiographic result with resolution of the stenosis and thrombus, but “slow reflow” was noted in the LAD, with significantly slower filling of the distal LAD compared with the circumflex artery (Figure 43-3 and Video 43-2). To treat the slow flow, the operator administered boluses of intracoronary adenosine via the guiding catheter, beginning with boluses of 50 mcg and increasing to 80 mcg as tolerated. Flow improved, although it remained abnormal. At this point, the operator treated the lesion with a 3.0 mm diameter by 18 mm long paclitaxel-eluting stent and further dilated it with 16 atmospheres inflation pressure using a 3.5 mm diameter by 15 mm long noncompliant balloon. Flow worsened after stenting (Figures 43-4, 43-5 and Videos 43-3, 43-4). Again, the operator administered multiple intracoronary boluses of adenosine via the guiding catheter, beginning with boluses of 50 mcg and increasing to 80 mcg as tolerated, until a total of 700 mcg had been administered. At the conclusion of the case, LAD flow was improved, although it had not returned to normal. The patient reported resolution of chest pain and remained hemodynamically stable, although persistent ST elevation was noted on the monitor and on a subsequent 12-lead ECG. The right femoral access sheath was removed with manual compression after 4 hours when the ACT measured less than 180 seconds but while the eptifibatide infusion was continuing.