CASE 42 Coronary Cavernous Fistula
Case presentation
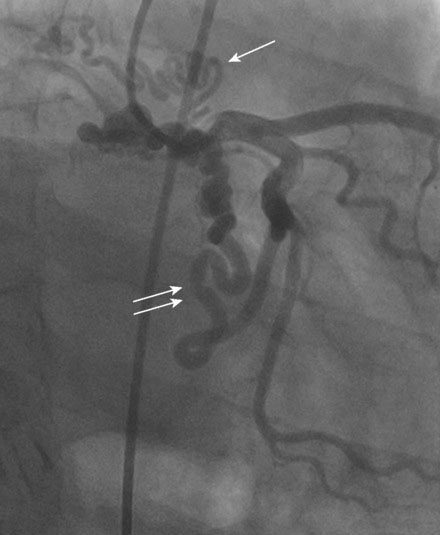
A 55-year-old man presented for management of a coronary cavernous fistula. One year prior to presentation, this otherwise healthy and active man with a history of hypertension, dyslipidemia, and obstructive sleep apnea developed progressive shortness of breath with exertion. This ultimately progressed to rest dyspnea and he presented to a local hospital with congestive heart failure requiring hospitalization. An echocardiogram found normal systolic function and no valvular abnormalities. Suspicious of coronary artery disease, his physician referred him for cardiac catheterization. To the operator’s surprise, the angiogram revealed a massive right coronary artery to right atrial fistula (Figure 42-1 and Video 42-1) and several fistulous connections from the left circumflex to the right atrium (Figure 42-2 and Video 42-2). The left anterior descending artery appeared normal, with no fistulae identified, and ventricular function was normal.

Cardiac catheterization
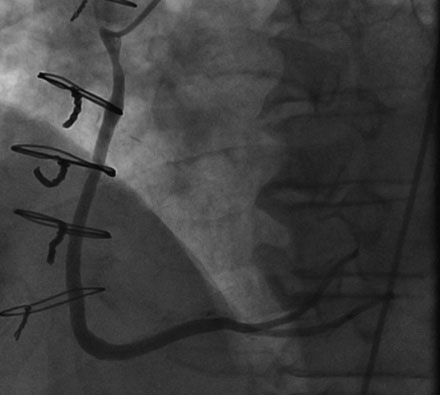
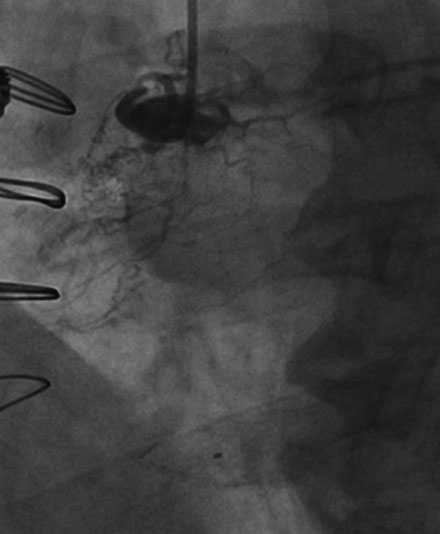
Right heart catheterization found fairly normal right sided pressures (mean right atrial pressure of 8 mmHg and pulmonary artery pressure of 27/5 mmHg). The oxygen saturation of blood sampled from the pulmonary artery was 67% with no evidence of a significant left-to-right shunt by oximetry. Cardiac output by the Fick method was 5.07 L/min. Angiography revealed wide patency of the vein graft to the right coronary (Figure 42-3) and continued exclusion of the fistula with no evidence of the fistula from the right coronary (Figure 42-4 and Video 42-3). The left coronary artery demonstrated a single fistulous connection to the right atrium (Figure 42-5 and Video 42-4) representing the distal fistula; the more proximal fistula previously noted was no longer evident.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


