CASE 40 Should a Nonculprit Artery Undergo PCI in the Setting of Acute STEMI?
Cardiac catheterization
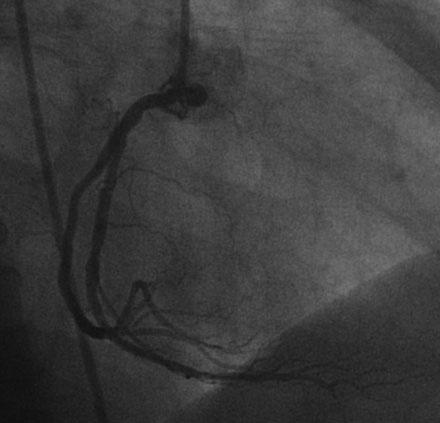
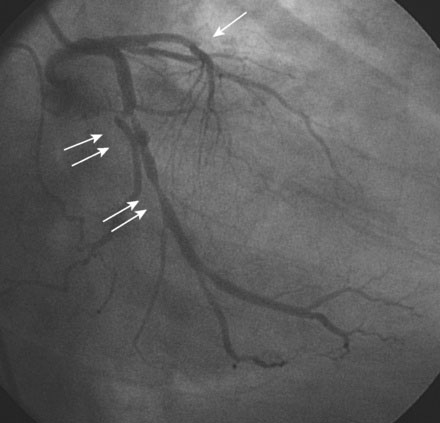
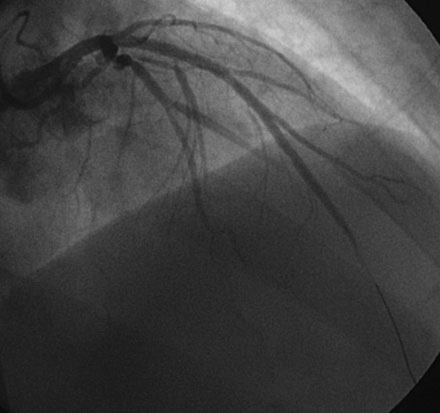
Hemodynamics obtained prior to coronary angiography revealed an elevated pulmonary capillary wedge pressure at 30 mmHg, elevated left ventricular end-diastolic pressure at 35 mmHg, a narrowed aortic pulse pressure, and tachycardia, consistent with the early phase of cardiogenic shock. Thus, the operator placed an intraaortic balloon pump for hemodynamic support. Angiography found a widely patent right coronary artery with mild luminal irregularities (Figure 40-1). Two consecutive severely narrowed tubular stenoses were present in a large, bifurcating, obtuse marginal branch of the circumflex artery. The LAD was occluded in its proximal portion just after the takeoff of a large septal branch (Figure 40-2 and Video 40-1). Anticoagulation was achieved with heparin and eptifibatide, and a 0.014 inch guidewire was easily advanced distally in the LAD. The lesion was predilated with a 2.5 mm diameter by 15 mm long compliant balloon with full balloon expansion and return of flow to the artery (Figure 40-3 and Video 40-2). Subsequently, a 3.0 mm diameter by 23 mm long sirolimus-eluting stent was placed successfully in the LAD with resultant TIMI-2 flow (Figure 40-4 and Video 40-3). His blood pressure remained low and he required a dopamine infusion (10 mcg/kg/min) for hemodynamic support. Given the patient’s deteriorating hemodynamic status, the operator was concerned about ongoing ischemia from the severe stenosis in the large circumflex artery and decided to perform percutaneous intervention on this vessel also. The 0.014 inch guidewire was removed from the LAD and advanced into the obtuse marginal. The sequential lesions were predilated with a 2.5 mm diameter by 15 mm long balloon with full balloon expansion. The distal lesion was treated with a 2.5 mm diameter by 13 mm long sirolimus-eluting stent, and a 3.0 mm diameter by 13 mm long sirolimus-eluting stent was deployed across the proximal lesion so there was overlap of the two stents. The final angiogram shows TIMI-3 flow in both the circumflex and LAD (Figure 40-5, and Video 40-4).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


