CASE 37 Inability to Stent in the Face of a Large Dissection
Cardiac catheterization
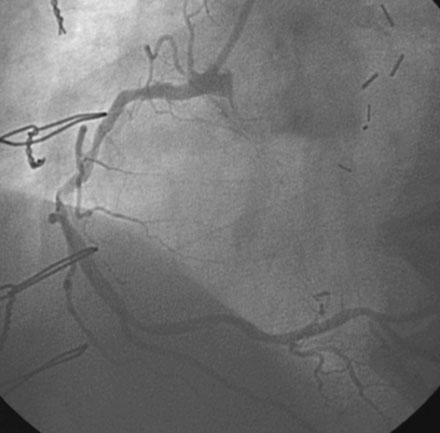
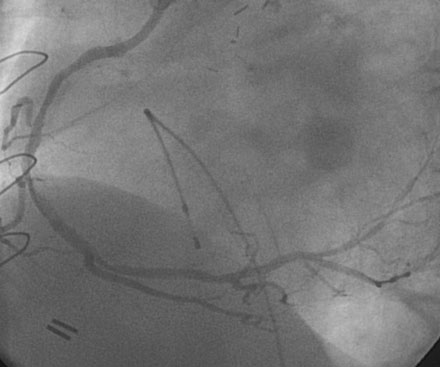
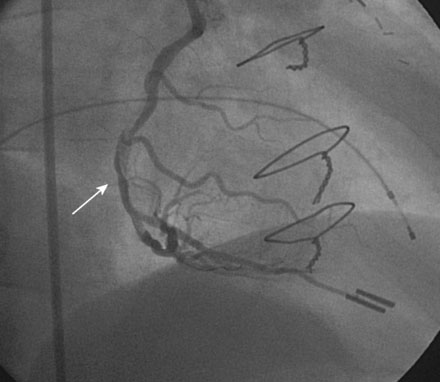
The left internal mammary graft to the LAD was intact and the LAD supplied collaterals to the circumflex (Video 37-1). The native LAD and circumflex were both occluded. Heavy calcification affected the right coronary artery and severe disease was present in the midsegment of this artery (Figures 37-1, 37-2 and Videos 37-2, 37-3). Because of extensive calcification, rotational atherectomy was planned. This was performed with a 1.5 mm burr through an 8 French right Judkins guide catheter after a temporary pacemaker was placed and procedural anticoagulation was achieved with unfractionated heparin and eptifibatide. Following rotational atherectomy, balloon angioplasty using a compliant, 2.5 mm diameter by 20 mm long balloon was accomplished at several locations within the mid-right coronary, and full inflation of the balloon was noted at nominal inflation pressures (Figure 37-3). The angiogram obtained after rotational atherectomy and balloon angioplasty is shown in Figures 37-4 and 37-5 and Videos 37-4 and 37-5. While the left anterior oblique projections appeared acceptable, the right anterior oblique projection revealed a large dissection in the midsection.


The operator then attempted to advance a stent (3.0 mm diameter by 20 mm long paclitaxel-eluting stent) to the mid-right coronary lesion with the goal of covering the entire dissection. However, the stent would not advance to the desired location. The operator decided to withdraw this stent and try a shorter, bare-metal stent; however, the first stent was firmly embedded in the lesion and would not withdraw to the guide. The operator feared that the stent might come off the balloon if additional force was applied and deployed the stent at the location, it became trapped (Figure 37-6). The angiogram obtained after this stent was deployed proximal to the desired location is shown in Figure 37-7. This stent was then aggressively postdilated with a noncompliant balloon and the unstented lesion in the midportion of the artery aggressively ballooned with a noncompliant balloon to high pressures after an additional and more supportive guidewire was placed as a “buddy” wire to facilitate another attempt at stent placement. The operator then chose a 3.0 mm diameter by 8 mm long bare-metal stent. With great difficulty, this stent was advanced distally, covering the distal part of the dissection (Figure 37-8
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


