CASE 35 Left Main Dissection
Case presentation
After presenting to the hospital with a 3-day history of intermittent chest pain and diaphoresis and found to have a non-ST segment elevation myocardial infarction, a healthy 49-year-old woman, with the coronary risk factors of tobacco abuse and dyslipidemia, underwent cardiac catheterization and was found to have a severe stenosis in the ramus intermedius branch (Figures 35-1, 35-2 and Video 35-1). Her other coronary arteries showed no angiographic evidence of significant atherosclerotic disease. She was subsequently referred for percutaneous treatment of the ramus intermedius branch.


Cardiac catheterization
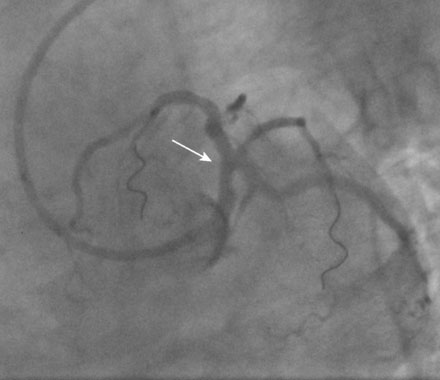
After passing the wire successfully and predilating the ramus lesion with a 2.0 mm diameter by 12 mm long compliant balloon, the operator happened to note an unexpected narrowing of the distal left main stem and positioned another 0.014 inch floppy-tipped guidewire into the left anterior descending artery (Figure 35-3 and Video 35-2). Several intracoronary boluses of nitroglycerin did not change the appearance of the distal left main narrowing. The physician proceeded with stenting of the ramus lesion using a 2.25 mm diameter by 16 mm long paclitaxel-eluting stent (Figure 35-4 and Videos 35-3, 35-4). The narrowing of the distal left main stem remained unchanged throughout the procedure on the ramus intermedius.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


