History
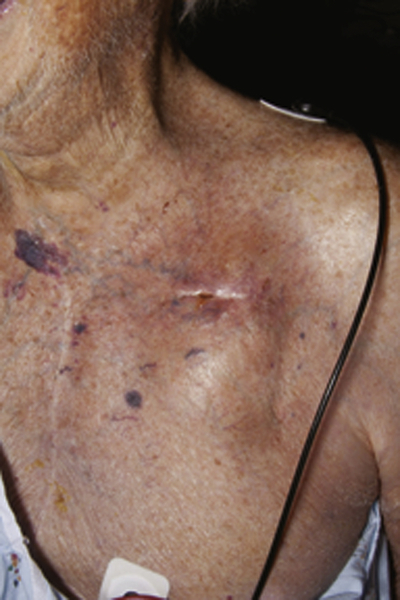
An 86-year-old gentleman was seen in the clinic for concerns regarding drainage at the site of his cardiac device on the left chest wall. His history was significant for ischemic heart disease and sinus node dysfunction, for which he had undergone pacemaker placement 2 years previously. At that time, his ejection fraction was estimated to be 38%. More recently, he was found to have New York Heart Association class III symptoms of congestive heart failure despite aggressive medical management. His ejection fraction was found to be 30%, and therefore his device was upgraded to a cardiac resynchronization therapy defibrillator (CRT-D) 6 weeks before presentation. At the time of this procedure, the old right ventricular pacing lead was removed but the chronic atrial lead was left in place. A routine recheck revealed the patient’s P wave to be significantly reduced, at 0.2 mV. Device interrogation confirmed that there was no capture on the atrial lead, and therefore he underwent atrial lead revision 3 weeks before presentation. This procedure was complicated by a postoperative hematoma at the surgical site that was managed conservatively. A few days after the procedure, he noticed pain, redness, and drainage from the device pocket in the left chest wall (Figure 35-1) and sought further evaluation at the clinic.
The review of systems in this patient was negative for fever or chills. He did have some fatigue and worsening shortness of breath but did not report chest pain or sputum production.
His other relevant comorbidities included prostate and laryngeal cancer, hypertension, hyperlipidemia, and iron deficiency anemia without an obvious source of bleeding. He had undergone a coronary artery bypass graft in 1994.
Current Medications
The patient was taking clopidogrel 75 mg daily, ferrous sulfate 325 mg (65 mg iron) daily, ramipril 5 mg daily, metoprolol 25 mg daily, isosorbide mononitrate 30 mg daily, furosemide 20 mg daily, niacin 1000 mg daily, simvastatin 40 mg daily, and aspirin 81 mg daily.
Current Symptoms
The patient was experiencing erythema, pain, and drainage at the site of device pocket in the left chest wall.
Physical Examination
Comments
Clinical examination shows dehiscence of surgical incision with purulent drainage and surrounding erythema consistent with cardiac device infection. The examination is also concerning for decompensated heart failure, as evidenced by increased jugular vein distention and peripheral edema.
Laboratory Data
Comments
Routine laboratory tests, including hemoglobin, leukocyte count, platelets, electrolytes, and inflammatory markers such as erythrocye sedimentation rate (ESR) and C-reactive protein (CRP) are neither sensitive nor specific for the diagnosis of cardiac device–related infection. The patient does have anemia and leukocytosis. These findings are not unexpected given the clinical history, which in itself is diagnostic of cardiac device infection.
Electrocardiogram
Findings
Normal sinus rhythm with biventricular pacing.
Comments
Electrocardiogram can provide clues to intracardiac complications of device-related infections such as conduction defects or heart block that may arise secondary to abscess formation.
Chest Radiograph
Findings
The chest radiograft revealed a small left pleural effusion with increased pulmonary vascularity and mildly increased perihilar prominence. Lungs were otherwise clear. Sternotomy wires and a left pectoral biventricular implanted cardiac device was seen.
Comments
Chest radiography can sometimes be helpful to detect septic emboli that arise as a result of dislodgement of lead vegetations. Our patient did not have these findings on his chest radiograph. Evidence of decompensated heart failure was present.
Echocardiogram



