CASE 30 Intracranial Hemorrhage After Coronary Intervention
Catheterization
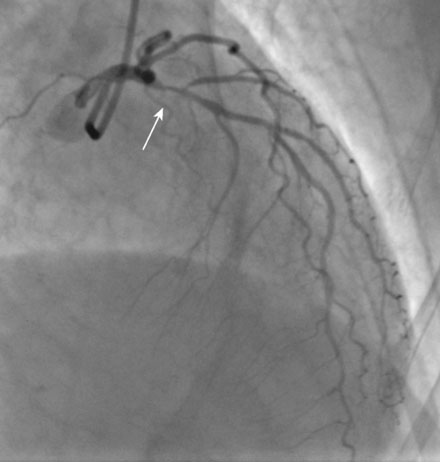
Left venticulography revealed mild anterior hypokinesis with preserved ejection fraction. Coronary angiography found no evidence of obstructive disease in the right or left circumflex coronary arteries. Severe atherosclerotic narrowing of the proximal segment of the left anterior descending artery was likely the explanation for her acute coronary syndrome (Figures 30-1, 30-2 and Videos 30-1, 30-2). Atherosclerosis also involved the first diagonal branch and the midsegment of the left anterior descending artery, but these lesions were felt to be nonobstructive. The lesion in the proximal segment of the left anterior descending artery was treated with balloon angioplasty followed by placement of a everolimus-eluting stent (2.5 mm diameter by 15 mm long) with an excellent angiographic result (Figure 30-3 and Video 30-3), and intravascular ultrasound confirmed stent apposition. The dose of enoxaparin planned for the morning of the procedure was held (last dose greater than 12 hours from catheterization) and procedural anticoagulation consisted of bivalirudin (33 mg intravenous bolus followed by an intravenous infusion of 1.7 mg/kg/hr) and 600 mg of clopidogrel administered orally at the time of the intervention. Hemostasis was achieved with a femoral artery closure device and she returned to a telemetry unit feeling well with no complaints.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


