CASE 3 Extensive Coronary Calcification
Case presentation
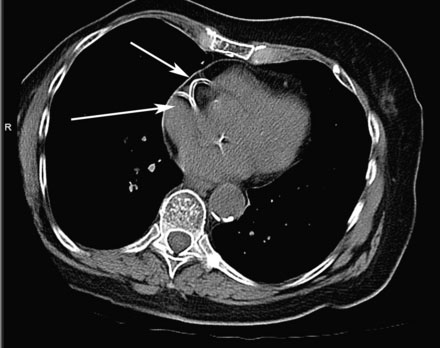
Three years following placement of a bare-metal stent in the right coronary artery, an otherwise active and healthy 85-year-old woman presented with the acute onset of sharp, stabbing anterior precordial chest pain radiating to the back. The pain was unrelieved by sublingual nitroglycerin and she presented to the hospital. Her only medications were aspirin 81 mg daily and atenolol 50 mg daily. Physical examination revealed a heart rate of 67 and a blood pressure of 110/54 mmHg and the remaining exam was unremarkable. In the emergency room, an electrocardiogram revealed nonspecific T wave inversion in lead III and initial cardiac biomarkers were not elevated. Because of the atypical nature of her chest pain and the absence of objective evidence of ischemia, she first underwent a CT angiogram of the chest to determine if her symptoms were due to an acute aortic dissection. This study showed no evidence of dissection but demonstrated extensive coronary and aortic calcification (Figure 3-1). She was admitted to a telemetry unit with a diagnosis of unstable angina, treated with enoxaparin, and underwent cardiac catheterization the next day.
Cardiac catheterization
Fluoroscopy confirmed the extensive coronary calcification in both the right and left coronary trees seen by CT scan (Figure 3-2). Despite heavy calcification, there was no significant luminal obstruction present in the left coronary artery on angiography. The right coronary artery, however, contained a complex, high-grade stenosis in the proximal segment, with extensive calcification (Figure 3-3 and Video 3-1).

FIGURE 3-2 This is a fluoroscopic image of the right coronary artery showing the heavy calcification present.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


