CASE 27 Loss of Side Branch During Right Coronary Intervention
Cardiac catheterization
Catheterization was performed during the hospital admission. Left ventricular function appeared normal and there was no significant disease noted in the left coronary artery (Figure 27-1); however, collateral filling of the distal right coronary artery was noted. The right coronary artery arose aberrantly high and anterior in the right coronary sinus. Heavy calcification along with severe atherosclerotic narrowing affected the midportion of the right coronary artery, and atherosclerotic disease also narrowed the ostium of the posterolateral side branch (Figures 27-2, 27-3 and Videos 27-1, 27-2).

FIGURE 27-1 This is a representative left coronary angiogram. There is no significant obstructive disease noted.
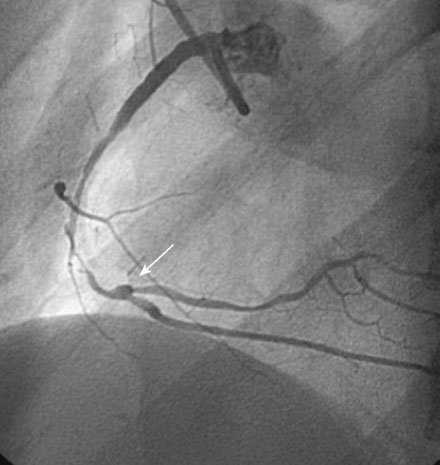

Her physician decided to proceed with percutaneous coronary intervention of the right coronary artery. Adequate backup for intervention required a left Amplatz 2.0 guide catheter. Procedural anticoagulation included intravenous bolus of heparin (50 U/kg) and double bolus plus infusion of eptifibatide using standard doses. The operator predilated the stenotic segment with a 2.5 mm diameter by 30 mm long compliant balloon, and chose bare-metal stents because of concern about the patient’s compliance with long-term clopidogrel. Two stents successfully treated the diseased segment with a 2.5 mm diameter by 18 mm long stent placed distally and a 3.0 mm diameter by 28 mm long stent deployed proximally (Figure 27-4 and Video 27-3). At this point, the ostium of the posterolateral branch appeared narrowed but remained patent. Noncompliant balloons (2.5 mm diameter by 20 mm long distally and 3.5 mm diameter by 15 mm long proximally) inflated to high pressure were used to postdilate the stented segment. Angiography after high-pressure balloon inflations demonstrated improved appearance of the stented segment but occlusion of the posterolateral side branch (Figures 27-5, 27-6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


