History
In September 2000 the patient was referred to a cardiologist because of premature ventricular contractions. The 12-lead surface electrocardiogram (ECG) showed sinus rhythm with atypical right bundle branch block (RBBB), a fragmented QRS, and negative T-waves in III, aVF and V1-3. Echocardiography, a 24-hour Holter ECG, and stress test were reported to be unremarkable. An expectant strategy was adopted.
In December 2009 the patient was hospitalized for sustained monomorphic ventricular tachycardia, with a heart rate of 254 bpm. A coronary angiogram did not show atherosclerosis. Magnetic resonance imaging (MRI) revealed marked thinning and hypokinesia of the basal anterior and anteroseptal wall. The left ventricular end-diastolic volume was 169 mL, left ventricular ejection fraction (LVEF) was 48%. Right ventricular volumes and systolic function were normal. An implantable cardioverter-defibrillator (ICD) was implanted, complicated by pneumothorax.
The patient experienced life-threatening electrical storm as a result of recurrent sustained monomorphic ventricular tachycardia in June 2010. When the emergency service arrived, the twelfth ICD shock was administered for monomorphic ventricular tachycardia resulted in ventricular fibrillation, and the patient lost consciousness. ICD therapy was disabled by a magnet and the patient resuscitated. After successful external defibrillation, acute ventricular tachycardia recurrence was prevented by intravenous amiodarone. However, despite amiodarone, ventricular tachycardia recurred during admission in her local hospital. The patient was referred for ventricular tachycardia ablation.
The patient’s cousin died suddenly at the age of 37. At autopsy a pale and mottled heart was found.
Comments
Although the ECG in 2008 was suspicious and the patient had symptomatic premature ventricular contractions, the echocardiogram, 24-hour Holter ECG, and stress test were reported to be unremarkable. However, contrast-enhanced MRI could have been considered at this time, based on the suspicious ECG.
Current Medications
The patient was taking thiamazole 30 mg daily, metoprolol Zoc 100 mg twice daily, calcium carbasalate (Ascal) 100 mg daily, ramipril 2.5 mg daily, oxazepam 10 mg three times daily, and clorazepate 5 mg if needed.
Current Symptoms
The patient received 12 ICD shocks for monomorphic ventricular tachycardia. In the hospital the patient was highly anxious because of the multiple ICD shocks. She did not report chest pain or dyspnea on exertion. The history was otherwise unremarkable.
Physical Examination
Laboratory Data
Electrocardiogram
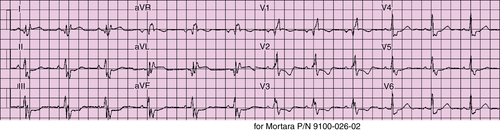
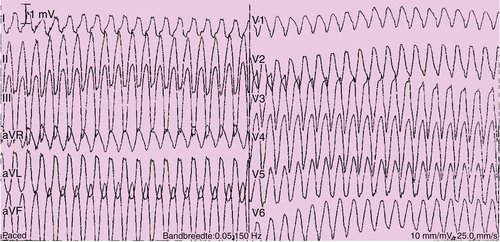
The ECG recorded sinus rhythm (Figure 26-1) and sustained monomorphic ventricular tachycardia (Figure 26-2) on the first day of admission at the cardiac care unit of the referring hospital.
Findings
The ECG in Figure 26-1 shows sinus rhythm at 72 bpm, pulse rate 140 ms, RBBB QRS 160 ms, QT/QTc 448/469 ms, a fragmented QRS with Q-waves in V1, I and aVL, a fragmented S-wave in lead II, V4 and V5, a fragmented R-wave in leads V2 and V3, and an R′ wave in leads I and aVL.
The ECG in Figure 26-2 recorded monomorphic ventricular tachycardia at 216 bpm, RBBB-like morphology (defined as dominant R in precordial lead V1), left superior axis, transition V3, and QRS width of 280 ms.
Echocardiogram
Findings
An echocardiogram of the left ventricle showed no hypertrophy, akinesia of the basal septum and basal anteroseptal wall, an end-diastolic volume of 170 mL, and LVEF of 35%. The right ventricle was not dilated and tricuspid annular plane systolic excursion was 25 mm.
Magnetic Resonance Imaging
Findings
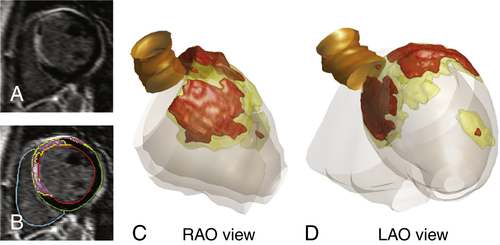
Based on cine magnetic resonance imaging (MRI) images, the LVEF was 40%, with marked hypokinesia of the basal anterior and anteroseptal wall, and the left ventricular end-diastolic volume was 182 mL. The right ventricle showed normal function and dimensions. The short-axis contrast-enhanced MRI slices (Figure 26-3, A) demonstrated a transmural scar in the basal anterior and anteroseptal wall. Using custom software, the contours were traced (see Figure 26-3, B) to create a three-dimensional scar reconstruction (see Figure 26-3, C and D).
Comments
The scar distribution is not typical for prior myocardial infarction, because the apical segments are completely spared. However, a scar distribution, involving in particular the basal septum and the adjacent basal anterior wall, has been previously described in patients with nonischemic dilated cardiomyopathy presenting with ventricular tachycardia.
Catheterization
The decision was made to perform ventricular tachycardia ablation to prevent recurrence of ventricular tachycardia and a potential life-threatening electrical storm. During endocardial ablation, multiple different ventricular tachycardia morphologies could be induced by programmed electrical stimulation (ventricular tachycardic cycle length 200 to 270 ms, most RBBB with inferior axis, one with RBBB and superior axis, and one with LBBB and superior axis). An electroanatomic map of the left ventricle was created, which revealed a low bipolar voltage area in the basal anteroseptal wall with fragmented electrograms, but no late potentials. For several episodes of ventricular tachycardia, early activation was identified in the basal left ventricle, but only 1 of 11 could be abolished. Although potential ablation target sites could be identified in close proximity to the bundle of His and the proximal left bundle, radiofrequency energy applications were withheld, considering that parts of the reentry circuits may be located deep intramurally or epicardially. The patient was rescheduled for a combined endocardial and epicardial procedure.