CASE 24 Early Stent Thrombosis
Case presentation
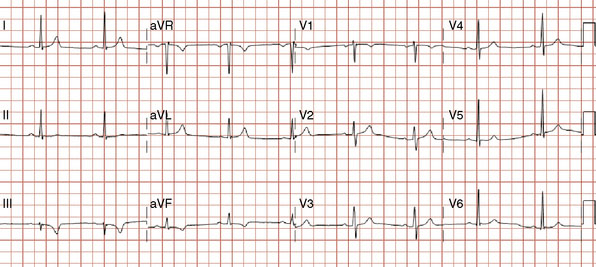
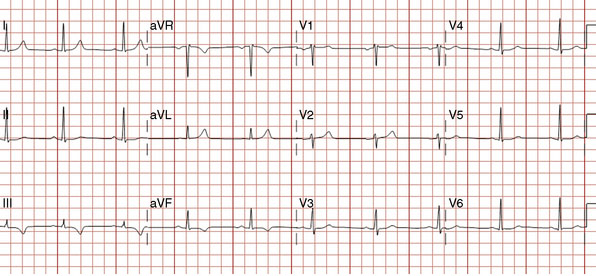
The onset of chest pain occurring during heavy exertion prompted a healthy 44-year-old man to seek medical attention. For 6 weeks, he had noted symptoms occurring only when running or performing strenuous labor. The chest pain always promptly resolved with rest. For many years he had maintained a high level of fitness for his job as a physical trainer, and he had no significant medical history except for a family history of premature coronary disease (both father and paternal grandfather suffered fatal acute myocardial infarctions at age 52 and 55, respectively). A 12-lead electrocardiogram was notable for T-wave inversions inferiorly (Figure 24-1). To further evaluate his symptoms, his family physician ordered an exercise stress test. He exercised to 12.9 METS but experienced chest pain in the third stage and developed 2 mm of downsloping ST-segment depression. His physician prescribed aspirin and metoprolol and referred him for cardiac catheterization.
Cardiac catheterization
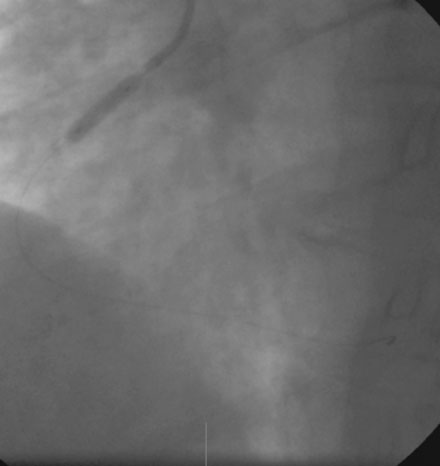
A severe stenosis present in the proximal right coronary artery explained his symptoms (Figure 24-2 and Videos 24-1, 24-2). Atherosclerotic disease evident in the left coronary artery did not appear to cause significant luminal obstruction (Figures 24-3, 24-4). The operator proceeded with percutaneous intervention of the right coronary artery using a bolus and infusion of bivalirudin as the procedural anticoagulant. The patient received 325 mg of aspirin prior to catheterization and was dosed with 600 mg of clopidogrel at the start of the percutaneous coronary intervention. Using first a 2.5 mm diameter by 20 mm long compliant balloon to predilate the lesion, the operator then deployed a 3.0 mm diameter by 23 mm long sirolimus-eluting stent (Figure 24-5). Not satisfied with the angiographic result, the operator postdilated the stent with a 3.0 mm diameter noncompliant balloon to 18 atmospheres (Figure 24-6). This resulted in a satisfactory angiographic result (Figure 24-7 and Videos 24-3, 24-4) and the patient left the cardiac catheterization laboratory without chest pain. An electrocardiogram obtained approximately 1 hour after the procedure showed no changes compared to baseline (Figure 24-8).

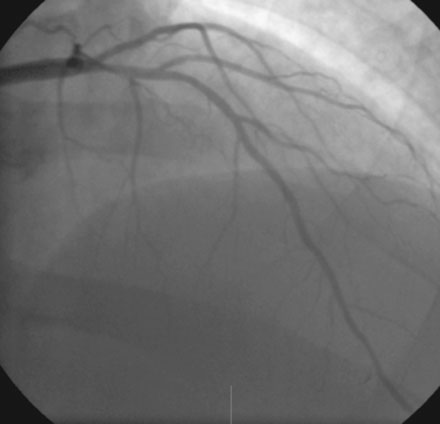
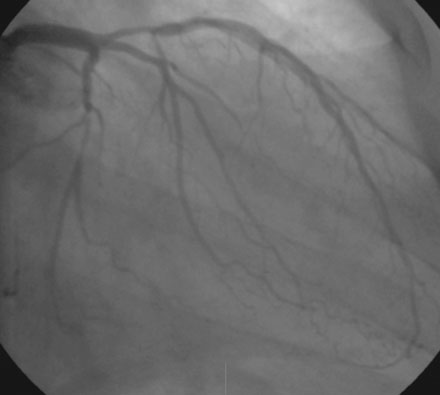

FIGURE 24-5 This angiogram was obtained following stent placement in the proximal portion of the right coronary artery.

Over the course of the afternoon, the patient reported continual low-grade chest discomfort, but repeat electrocardiograms showed no changes. Although the pain was attributed to noncardiac causes, it continued throughout the afternoon and failed to respond to nitrates, antacids, or positional changes. Approximately 6 hours after the intervention, the chest pain suddenly became acutely worse and was associated with diaphoresis, nausea, and bradycardia. An electrocardiogram obtained at this point revealed normalization of the previously present inferior T-wave changes and new ST-segment elevation in leads III and aVF (Figure 24-9). Emergency coronary angiography confirmed occlusion of the right coronary stent (Figure 24-10 and Video 24-5).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


