CASE 22 Saphenous Vein Graft Rupture
Cardiac catheterization
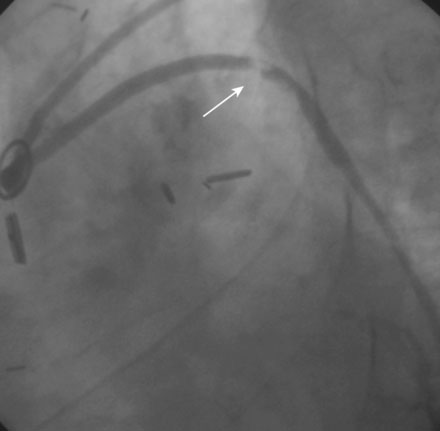
Angiography found wide patency of both internal mammary artery grafts and a severe proximal stenosis and moderately severe, more distal stenosis in the body of the 14-year-old vein graft to the obtuse marginal artery (Figures 22-1, 22-2 and Videos 22-1, 22-2). The operator planned to stent both the proximal and midgraft lesions with distal embolic protection afforded by the PercuSurge Guardwire (Medtronic) temporary balloon occlusion and aspiration system.1 An 8 French, right Judkins guide catheter was inserted in the vein graft. The operator chose unfractionated heparin and eptifibatide for procedural anticoagulation, and the Guardwire was positioned distally in the vein graft. The occlusion balloon was inflated to allow distal embolic protection. After first dilating with a 3.5 mm diameter balloon, a 4.5 mm diameter by 18 mm long bare-metal stent was deployed in the proximal lesion (Figure 22-3). The operator then positioned and deployed a 4.0 mm diameter by 28 mm long bare-metal stent in the midgraft lesion. Aspiration was performed, the distal occlusion balloon deflated, and angiography performed. To the operator’s horror, free-flowing contrast was observed extravasating from a large defect in the midportion of the vein graft within the stented segment (Video 22-3). The patient developed marked hypotension with arterial pressure falling to 50/30 mmHg. To staunch the hemorrhage, a 3.5 mm perfusion balloon was positioned and inflated in the vein graft at the site of the defect, eptifibatide was discontinued, and 30 mg of protamine was administered intravenously. This greatly decreased the amount of contrast extravasation, and the perfusion balloon allowed distal perfusion; however, there remained evidence of ongoing hemorrhage by angiography (Video 22-4). Fluid resuscitation and dopamine infusion restored blood pressure, but each time the balloon was deflated for even a few seconds, the patient developed marked hypotension. Since the operator did not feel there was sufficient time to safely exchange the perfusion balloon for a PTFE-covered stent nor felt confident that the large defect could be successfully sealed with this device, cardiothoracic surgery agreed to operate on the patient emergently.