History
A 68-year-old man previously underwent implantation of a cardiac resynchronization therapy defibrillator (CRT-D) device (February 2007) after a class I indication for CRT at the time—symptomatic drug-refractory ischemic-based heart failure disease, New York Heart Association (NYHA) class III, severe left ventricular dysfunction, and left bundle branch block (LBBB) ventricular conduction delay, with a 130-msec duration QRS complex. Despite CRT, clinical follow-up of the patient was characterized by gradually worsening heart failure progression with further reduction of left ventricular function (left ventricular ejection fraction [LVEF] <20%), dilation of the left ventricle, and, as a result of dilation of the mitral annulus, progression of mitral regurgitation to grade III. Therefore the patient underwent successful positioning of a MitraClip (Abbott Vascular, Abbott Park, Ill.) device in September 2009, thus achieving mitral regurgitation reduction to grade I or II. Paroxysmal atrial fibrillation gradually progressed to become permanent, and ablation of the atrioventricular node was performed to achieve adequate CRT delivery. Other comorbidities included chronic renal insufficiency (reduced glomerular filtration rate of 40 to 50 mL/min/1.73 m2), previous nephrectomy for renal papillary carcinoma, and hyperuricemia.
Because of persistent severe heart failure symptoms (NYHA class IIII to IV), in May 2011 the patient consented to participate in a prospective multicenter safety and feasibility study evaluating a wireless cardiac stimulation system of the left ventricular endocardium (wireless cardiac stimulation cardiac resynchronization therapy [WiCS-CRT]).
Current Medications
At presentation, the patient’s therapeutic scheme included maximally tolerated dosages of beta blocker, an angiotensin-converting enzyme [ACE] inhibitor, and other relevant drugs: clopidogrel 75 mg daily, acenodecumerol 1 mg to maintain international normalized ratio between 2 and 3, carvedilol 12.5 mg daily, enalapril 40 mg daily, spironolactone 25 mg daily, atorvastatin 40 mg daily, and aspirin 100 mg daily.
Current Symptoms
The patient exhibited breathlessness at mild exertion and had NYHA class III to IV heart disease.
Physical Examination
Laboratory Data
Electrocardiogram
Findings
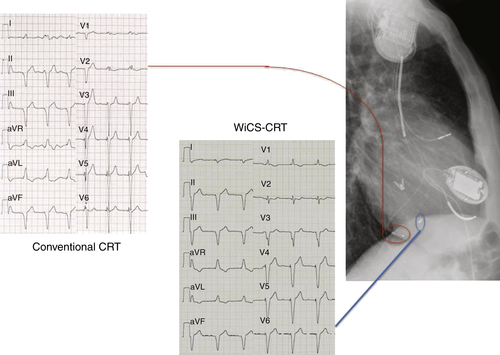
The electrocardiogram of conventionally delivered CRT is shown in Figure 20-1 (left panel). Vertical QRS axis (160 msec) coupled with R wave in V1 indicates regular epicardial biventricular pacing in VVI modality at 70 bpm. Left ventricular stimulation from a bipolar left ventricular tip positioned in a postero-lateral branch of the coronary sinus (red circle) confers a vertical axis to the QRS complex and QS morphology in the inferior leads.
Chest Radiograph
Findings
Anteroposterior and right lateral (Figure 20-2, upper panels) show the positioning of the three leads with the transvenous left ventricular lead positioned in a posterolateral branch of the cornonary sinus (red circle) and reaching a posterolateral apical position.
Echocardiogram
Findings
At baseline, echocardiographic examination revealed a severely dilated left ventricle with diffuse hypokinesia and highly compromised left ventricular function (LVEF 19%). Despite MitraClip implantation, residual moderate mitral insufficiency was present; moderate tricuspid insufficiency was also present (Figure 20-3, left panel, and video left panel). Pulmonary pressures were increased, with an estimated arterial pulmonary pressure of 40 mm Hg (see video baseline).
Focused Clinical Questions and Discussion Points
Question
What is the pathophysiologic basis for considering left ventricular endocardial pacing to deliver CRT?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


