Chapter 20
Questions
- 381. The commonest location of this pathology is:
- A. Proximal ascending aorta
- B. Midaortic arch
- C. At the attachment of ligamentum arteriosum
- D. Junction of thoracic and abdominal aorta
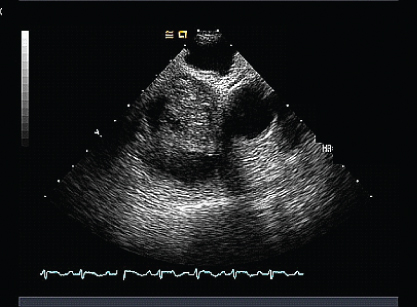
- 382. This is a 27-year-old man with no prior medical history, presented with a three-month history of abdominal distension and lower extremity edema. Physical examination revealed severely elevated jugular venous pressure. He had normal left ventricular (LV) and right ventricular (RV) systolic functions. The most likely diagnosis is:
- A. Superior mediastinum syndrome
- B. Constrictive pericarditis
- C. Restrictive cardiomyopathy
- D. Cirrhosis of the liver
- 383. This patient presented with shortness of breath and cyanosis. The most likely cause is:
- A. Ventricular septal defect (VSD) with Eisenmenger’s
- B. Atrial septal defect (ASD) with Eisenmenger’s
- C. Tetralogy of Fallot
- D. Primary pulmonary hypertension
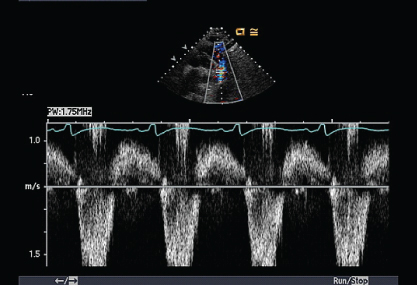
- 384. This pulmonary regurgitation (PR) signal is suggestive of:
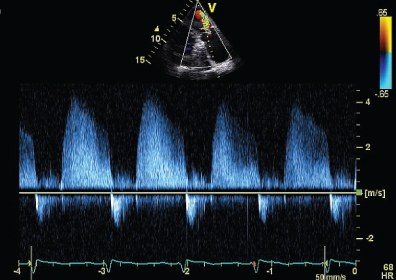
- A. Severe pulmonary hypertension
- B. Mild pulmonary hypertension
- C. Normal pulmonary artery (PA) pressure
- D. Severe pulmonic stenosis
- B. Mild pulmonary hypertension
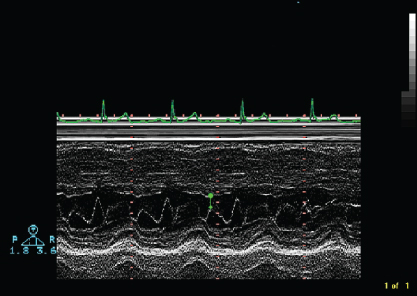
- 385. The Doppler signals shown here are indicative of:
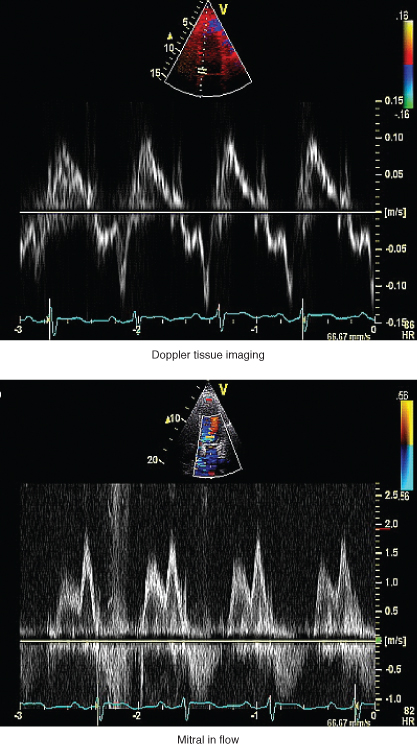
- A. Normal LV diastolic function
- B. Abnormal LV relaxation with probable elevated left atrial (LA) pressure
- C. Abnormal LV relaxation with probably normal LA pressure
- D. Advanced restrictive cardiomyopathy
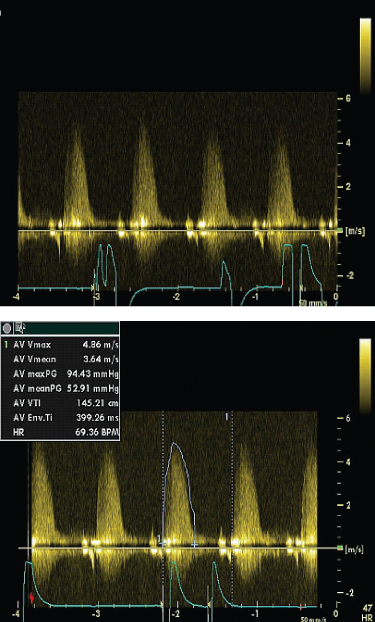
- 386. The continuous wave Doppler signal shown here is suggestive of:
- A. Dynamic LV outflow obstruction due to systolic anterior motion (SAM)
- B. Critical valvular aortic stenosis (AS)
- C. Subvalvular AS due to a membrane
- D. Flow in and out of pseudoaneurysm
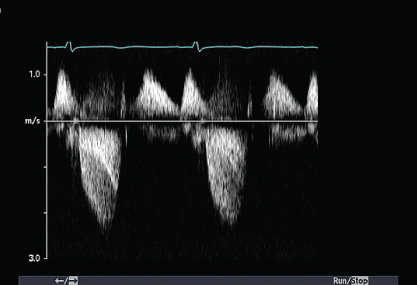
- 387. This signal was obtained from a right upper parasternal location with the patient turned to the right using a dedicated continuous wave Pedoff transducer. The likely diagnosis is:
- A. Severe mitral regurgitation (MR)
- B. Severe tricuspid regurgitation (TR)
- C. Severe AS
- D. None of the above
- B. Severe tricuspid regurgitation (TR)
- 388. The aortic valve shown in this image is:
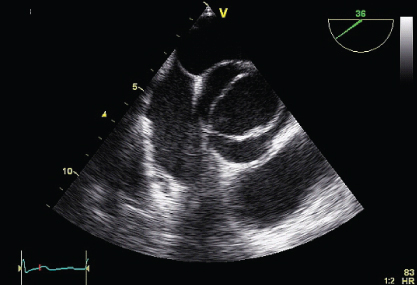
- A. Unicuspid
- B. Tricuspid
- C. Bicuspid
- D. Quadricuspid
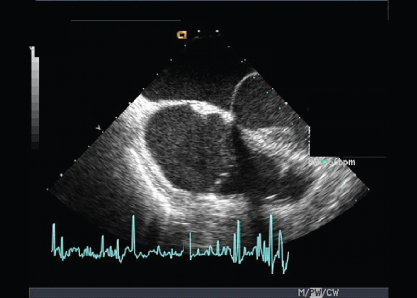
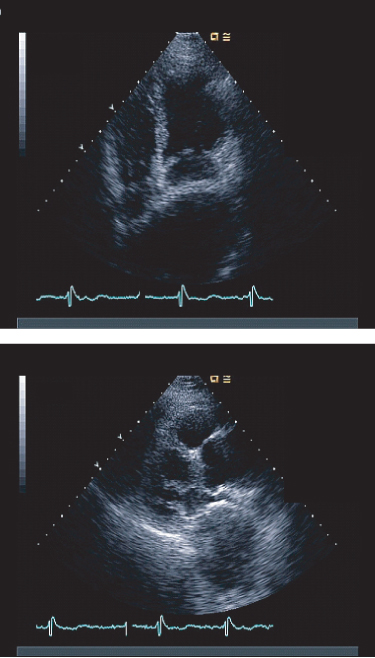
- 389. A 32-year-old female with complaints of shortness of breath, pedal edema, flushing, and diarrhea had an echocardiogram. The representative end systolic and end diastolic frame of an RV inflow view is shown. What does the patient have?
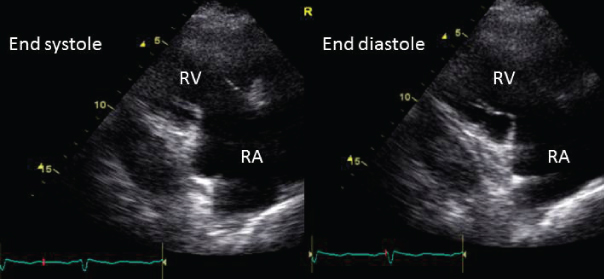
- A. Tricuspid valve prolapse potentially causing severe TR
- B. Rheumatic involvement of the tricuspid valve
- C. Carcinoid involvement of the tricuspid valve
- D. None of the above
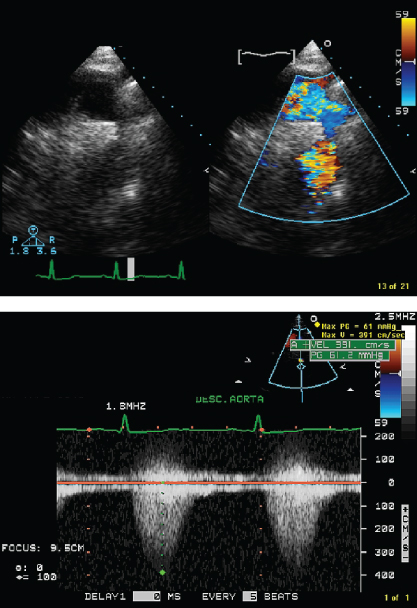
- 390. This flow obtained from the distal aortic arch from the suprasternal notch is indicative of:
- A. Severe AR
- B. Aortic coarctation
- C. Severe AS
- D. None of the above
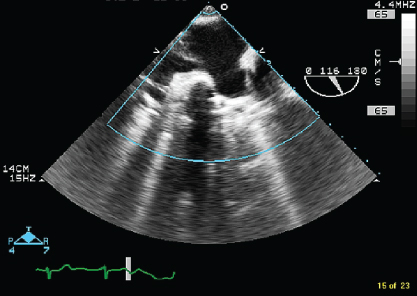
- 391. This image of the LV is indicative of:
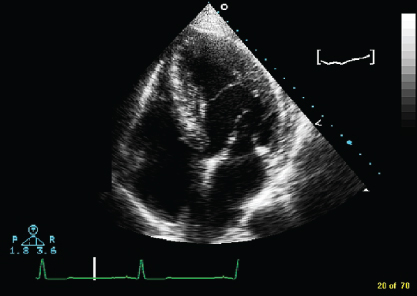
- A. An LA thrombus
- B. Left ventricular noncompaction
- C. Bilobed LV
- D. False tendon
- 392. Saline contrast echocardiography is suggestive of:
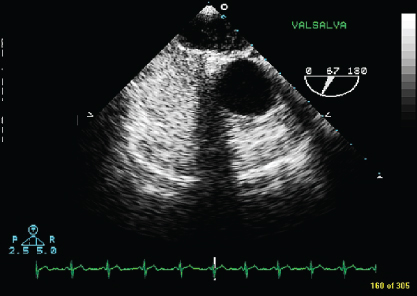
- A. Patent foramen ovale (PFO)
- B. Pulmonary AV fistula
- C. Patent foramen or pulmonary A–V fistula
- D. No right-to-left shunting
- 393. This transesophageal echocardiogram (TEE) image from the upper esophageal location shows:
- A. Left atrial appendage
- B. Left upper and lower pulmonary veins
- C. Left and right atria
- D. Pulmonary artery branches
- 394. These two images obtained from the suprasternal notch are diagnostic of:
- A. Coarctation of the aorta
- B. Patent ductus arteriosus
- C. Normal aortic flow
- D. Pulmonary artery branch stenosis
- 395. This TEE image is indicative of:
- A. Left atrial myxoma
- B. Right atrial myxoma
- C. Lipomatous atrial septum
- D. Vegetation of the tricuspid valve
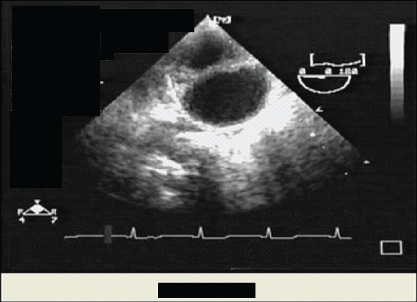
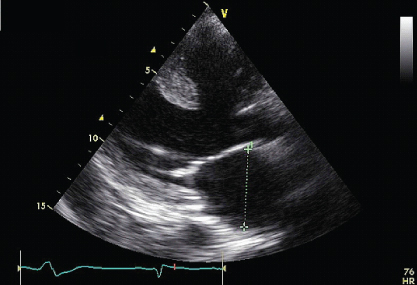
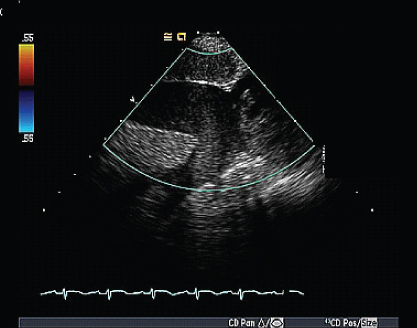
- 396. What is the abnormality seen on this transthoracic echocardiogram?
- A. Aneurysmal left atrium
- B. Partial absence of the pericardium
- C. Thoracic aortic aneurysm
- D. Loculated pleural effusion
- B. Partial absence of the pericardium
- 397. The amount of MR in this patient is likely to be:
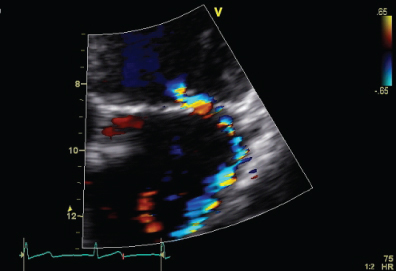
- A. 1+
- B. 2+
- C. 3 or 4+
- D. Cannot quantify
- 398. The cause of the systolic murmur in this patient is likely to be:
- A. Rheumatic MR
- B. Valvular AS
- C. Hypertrophic obstructive cardiomyopathy (HOCM)
- D. Aortic subvalvular membrane

Stay updated, free articles. Join our Telegram channel
- A. Proximal ascending aorta

Full access? Get Clinical Tree


