19: Parenchymal Lung Disease and Chronic Thromboemboli
Figure 19.1
CT angiogram of the chest obtained at initial presentation
The patient presented again 7 years later with dyspnea. He noted initial improvement in his respiratory symptoms after his discharge from the previous hospitalization; however, the improvement was short-lived. He was now limited to climbing less than a flight of stairs without stopping and he was sharing farm chores with his sons due to his limitations. His 6 min walk distance at that time was 209 m with a BORG dyspnea score of 10. He denied chest pain, lightheadedness and near syncope. He had lower extremity edema (right leg > left leg). Vital signs upon consultation demonstrated a blood pressure of 122/70 mmHg and a SaO2 of 93% on 4 L/min. His BMI was 26 kg/m2. His chest exam was notable for end-expiratory wheezes bilaterally. His cardiovascular exam noted a jugular venous pressure of 8 cm, a normal S1 and S2 and no appreciable murmurs. Pulmonary function tests revealed severe obstruction with a forced expiratory volume (FEV1) = 1.1 L (35%) and a diffuse capacity adjusted for hemoglobin (DLCO) of 10.3 mL/mmHg/min (33% predicted). Forced vital capacity was 3.76 L (92%). His echocardiogram showed a mildly dilated right ventricle and an insufficient tricuspid regurgitant jet to estimate a right ventricular systolic pressure (RVSP) estimate. Laboratory assessment showed normal α-1 antitrypsin levels, a non-reactive antinuclear antibody, normal thyroid stimulating hormone and no evidence of hepatitis C virus or human immunodeficiency virus. Chest x-ray (Fig. 19.2) demonstrated flat hemidiaphragms, increased lung volumes and dilated intralobar pulmonary arteries: Past medical history was notable for emphysema and systemic hypertension .
Figure 19.2
PA and lateral chest radiograph
On social history, the patient has 5 healthy children. He worked as a welder and in the oil fields. He currently runs a small farm with horses and cows only. He has a 12 pack-year tobacco history and quit 20 years ago. He does not drink alcohol. There is no history of methamphetamine, cocaine or fenfluramine exposures. Family history was notable for a father and brother with emphysema.
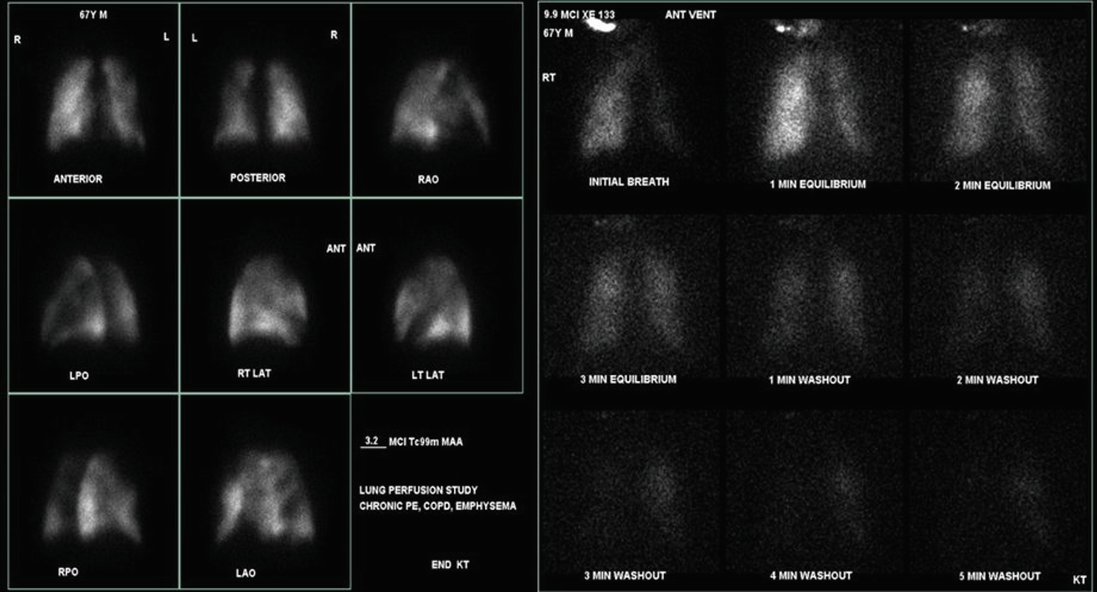
Given the previous history of pulmonary embolism, a ventilation-perfusion scan was obtained. The study showed multiple moderate or large segmental perfusion defects throughout both lungs. Ventilation images showed xenon retention (Fig. 19.3).
Figure 19.3
Lung scintigraphy showing both ventilation and perfusion abnormalities
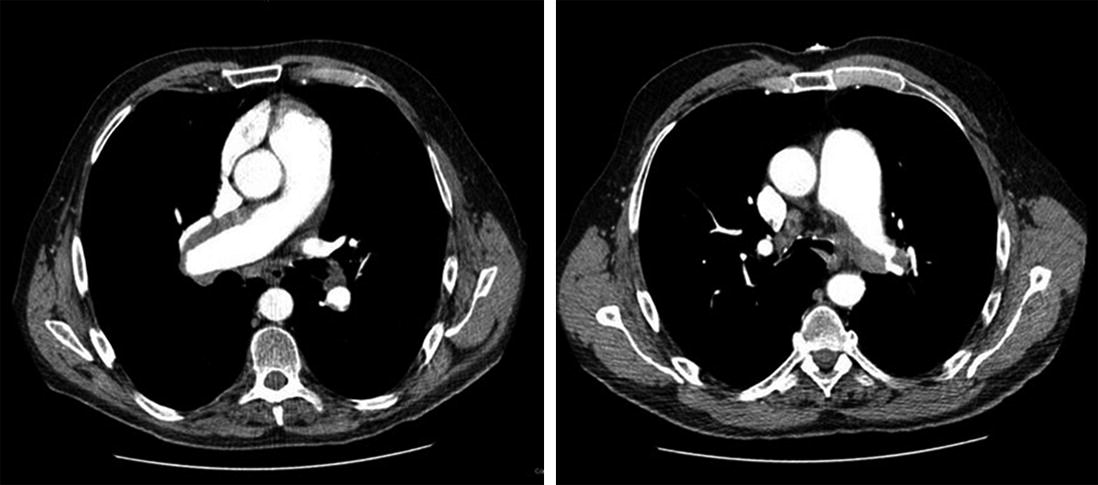
Further assessment was obtained via CT pulmonary angiogram (Figs. 19.4 and 19.5).
Figure 19.4
Follow up CT angiogram of the chest reveals lining thrombus involving the central pulmonary arteries
Only gold members can continue reading. Log In or Register to continue