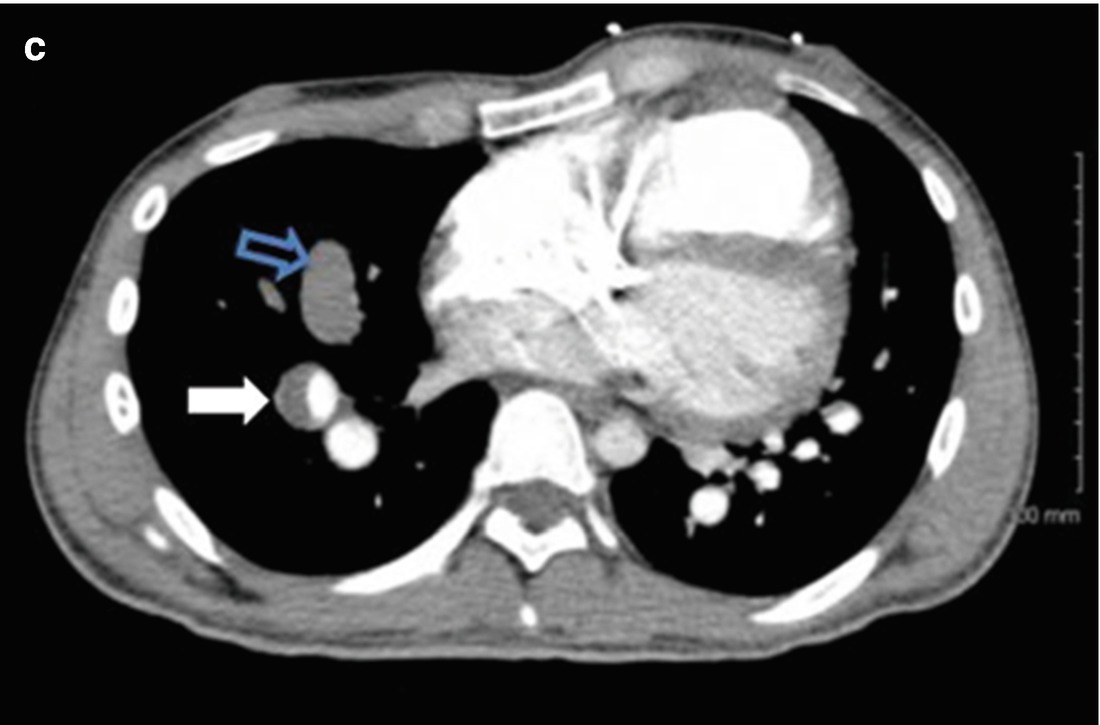
CTA of the chest showing occlusive thrombus in a left upper lobe (panel b, blue arrow) and right middle lobe pulmonary artery (panel c, open blue artery). Eccentric lining thrombus in a markedly enlarged right main PA, and in dilated left upper lobe, right lower lobe segmental vessels also noted (panels a, c, white arrows)

Chest radiography (AP view) demonstrates cardiomegaly with aneurysmal dilatation of the proximal pulmonary arteries. There is no obvious pulmonary artery calcification
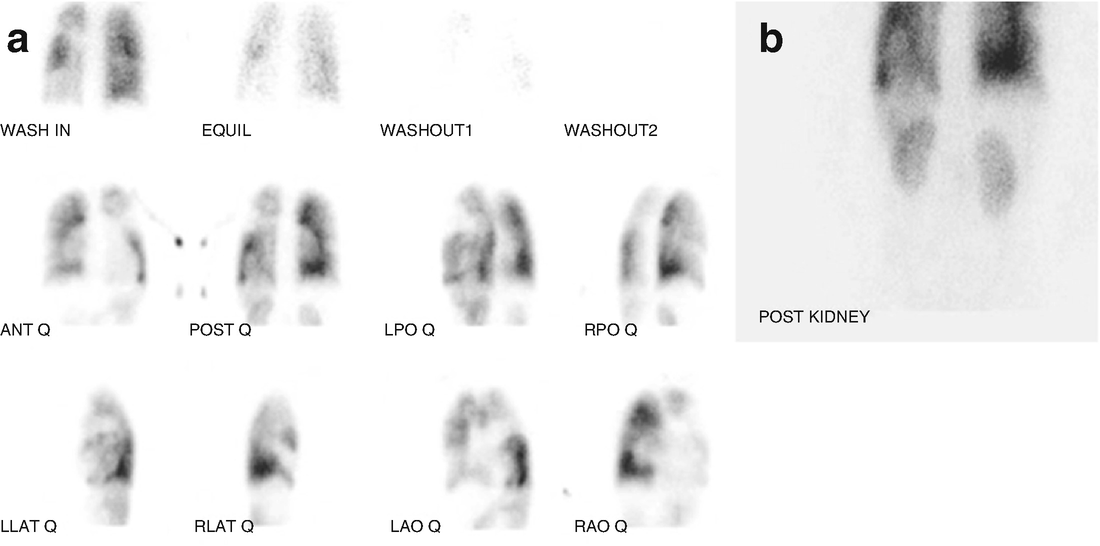
Lung scintigraphy showing unmatched perfusion defects (panel a) as described in the text, with uptake evident in the kidneys suggesting a right to left shunt (panel b)
Saturation Run: Systemic pulse oximetry 82–84%, high SVC saturation 45%, low SVC saturation 44%, mid RA saturation 62%, IVC saturation 46%, right ventricle saturation 61%, PA saturation 59%.
Baseline hemodynamics:
Mean right atrial pressure of 2.
Right ventricular systolic pressure of 88, right ventricular end-diastolic pressure of 4.
Pulmonary artery pressure 92/51, mean pulmonary artery pressure 64.
Pulmonary capillary wedge pressure 4.
Cardiac output calculations: Qs was equal to 2.17 L/min with cardiac index of 1.4 m−2. Qp was calculated using a few assumed pulmonary venous saturations. Assuming a pulmonary venous saturation of 95%, Qp was equal to 2.36 L/min, 1.5 m−2.
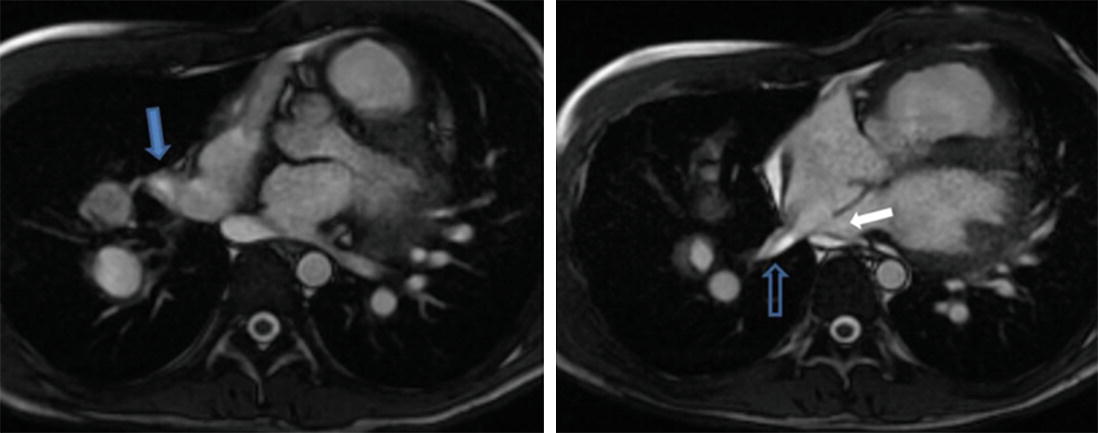
Cardiac magnetic resonance imaging (axial view) depicting right superior (solid blue arrow) and right inferior (open blue arrow) pulmonary veins draining into the right atrium. Sinus venosus defect: white arrow
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


