17: Can Severe Pulmonary Arterial Pulmonary Hypertension Mimic CTEPH?
Figure 17.1
Chest X-raywith normal heart size and no significant parenchymal abnormalities
Because of significant symptoms, further assessment was pursued. Echocardiogram was notable for normal systolic left ventricular (LV) function with ejection fraction of 55%. Right ventricle was mild to moderately dilated. Tricuspid valve was moderate to severely regurgitant and pulmonary pressures were estimated at 78 mmHg.
His abnormal echocardiogram prompted further evaluation of the etiology and severity of his elevated pulmonary pressures. Additional laboratory assessment revealed normal thyroid function and no significant abnormalities on autoimmune workup. Pulmonary function testing (Table 17.1) did not reveal significant changes that could account for severity of elevated pulmonary pressures.
Table 17.1
Pulmonary function test without significant obstruction or restriction. Diffusing capacity was mildly decreased
FEV1 (L)
2.96
FEV1%
89
FVC (L)
4.31
FVC%
92
FEV1/FVC (%)
69
TLC (L)
6.56
TLC%
98
RV
1.52
RV%
65
VC
5.04
VC%
1.08
DLCO (mL/mmHg s)
19.5
DLCO %
78
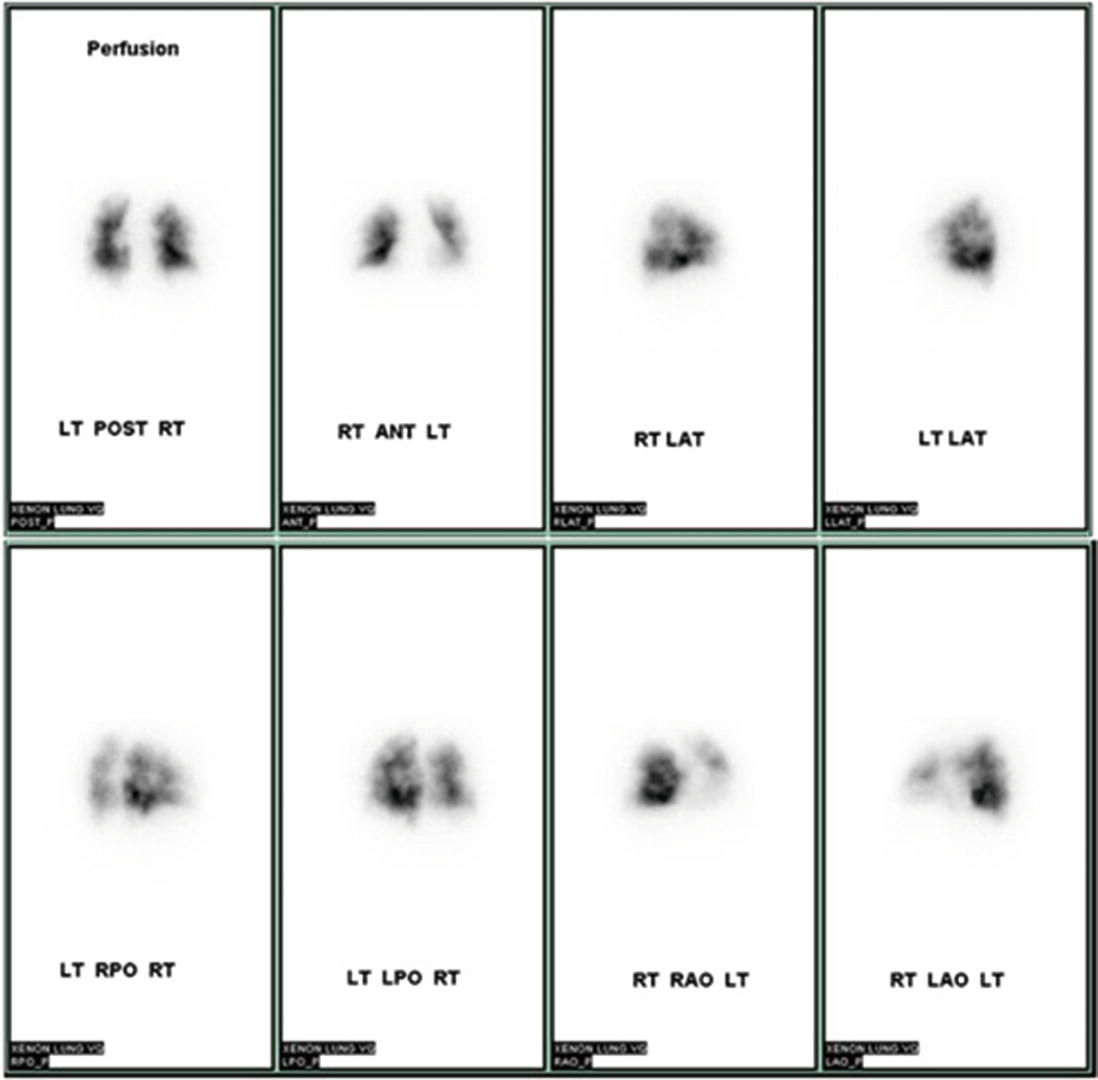
Additional imaging was performed to assess for possibility of pulmonary embolism as etiology of his progressive shortness of breath and echocardiographic findings. Ventilation (Fig. 17.2)/perfusion (Fig. 17.3) scanning was performed and revealed bilateral patchy perfusion defects without significant ventilation abnormalities.
Figure 17.2
Xenon ventilation scanning with symmetric ventilation and mild bilateral retention
Figure 17.3
Ventilation/perfusion scanning with significant bilateral patchy perfusion defects
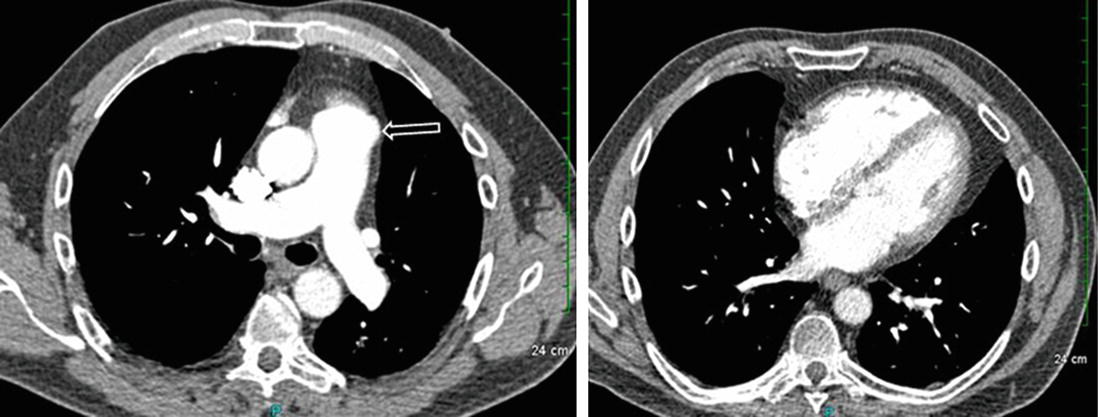
Based on V/Q, there was concern for chronic thromboembolic pulmonary hypertension (CTEPH). A more definitive evaluation with CT pulmonary angiogram (CTPA) (Fig. 17.4) was therefore requested. CTPA revealed enlarged pulmonary arteries but no evidence of significant parenchymal lung disease or pulmonary emboli.
Figure 17.4
CT chest with pulmonary angiography revealed enlarged pulmonary arteries (arrow) without evidence of acute or chronic pulmonary emboli
Only gold members can continue reading. Log In or Register to continue