CASE 14 Extensive Coronary Thrombus
Cardiac catheterization
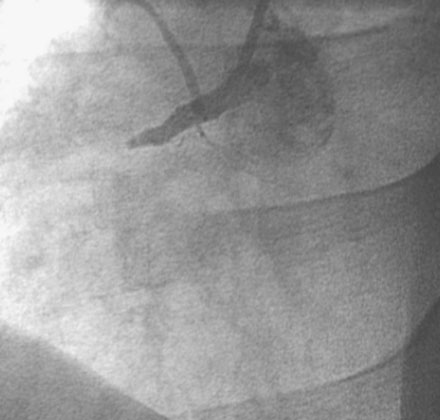
The patient arrived in the cardiac catheterization laboratory approximately 2 hours after receiving thrombolysis. As expected, the right coronary artery was completely occluded (Figure 14-1). There was no significant obstructive disease noted in the left coronary arteries. An additional intravenous bolus of enoxaparin was administered, along with a bolus plus infusion of eptifibatide. The operator inserted a guide catheter and easily passed a 0.014 inch floppy-tipped guidewire to the distal artery. A 2.5 mm by 20 mm long compliant balloon inflated at the occlusion site immediately restored TIMI-3 flow, and resulted in resolution of chest pain and ST-segment elevation. However, an extensive filling defect was observed, consistent with a large intracoronary thrombus (Figure 14-2 and Video 14-1). The operator passed a Pronto extraction catheter over the floppy-tipped guidewire to the distal artery and, using a 30 cc syringe, gently aspirated as the catheter was withdrawn to the guide catheter. A large amount of clot was successfully removed and improved the angiographic appearance of the artery with no evidence of distal embolization (Figure 14-3 and Video 14-2). A 4 mm diameter by 28 mm long bare-metal stent postdilated with a 4.5 mm noncompliant balloon successfully treated the residual stenosis (Figures 14-4, 14-5 and Video 14-3). At the completion of the procedure, the patient had no further chest pain and was transferred to the coronary care unit.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


