CASE 13 Complex Coronary Disease
Case presentation
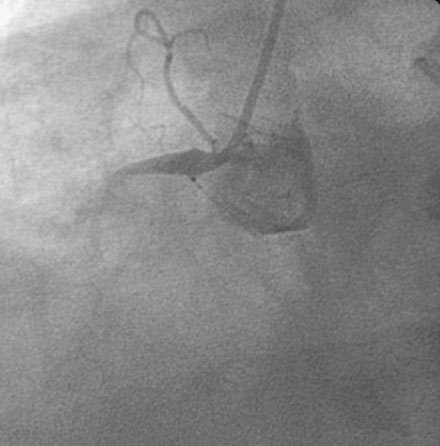
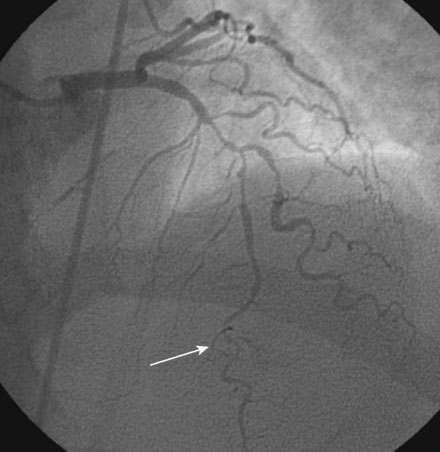
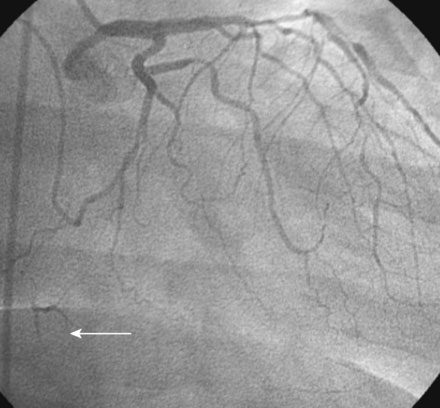
The onset of severe substernal chest pain awakened a 50-year-old diabetic woman without prior cardiac history from her sleep. The pain waxed and waned all morning until she finally presented to the emergency room 9 hours later. She was found to have an inferior wall ST-segment elevation myocardial infarction and was taken emergently to the cardiac catheterization laboratory. As suspected, based on the electrocardiographic changes, the right coronary artery was completely occluded (Figure 13-1); however, the operator was surprised to find severe and complex disease affecting the left anterior descending (LAD) and diagonal arteries (Figure 13-2 and Video 13-1) and moderate disease in the left circumflex artery (Figure 13-3 and Video 13-2). Lush collaterals filled the distal right coronary artery from the left coronary injections.
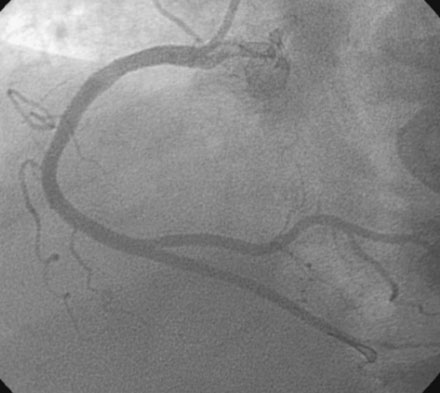
With the goal of achieving rapid reperfusion of the infarct-related artery, the operator decided to open the right coronary artery. This was promptly and successfully accomplished with balloon angioplasty followed by deployment of two 4.5 mm diameter bare-metal stents. The operator obtained an excellent luminal result and TIMI-3 flow (Figure 13-4 and Video 13-3).
Cardiac catheterization
She returned to the cardiac catheterization laboratory for an elective complex intervention of the LAD and diagonal. After achieving therapeutic anticoagulation, the operator advanced 0.014 inch floppy-tipped guidewires in both the LAD and diagonal and performed balloon angioplasty in the LAD with a 2.0 mm diameter by 20 mm long compliant balloon (Figure 13-5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


