12: Pulmonary Veno-Occlusive Disease …but It Started Out as CTEPH
Figure 12.1
CT angiography shows prominent perivascular and subcarinal tissue
An evaluation for pulmonary arterial hypertension was initiated given history and echocardiographic findings. Serological screening for connective tissue disease in the form of antinuclear antibody (ANA) and rheumatoid factor (RF) were negative. Human immunodeficiency virus (HIV) testing was negative. Pulmonary function testing was consistent with a restrictive pattern as evidenced by FVC 60% predicted, FEV1 57% of predicted, FEV1/FVC 77, TLC 63% of predicted and DLCO was significantly reduced at 38% of predicted.
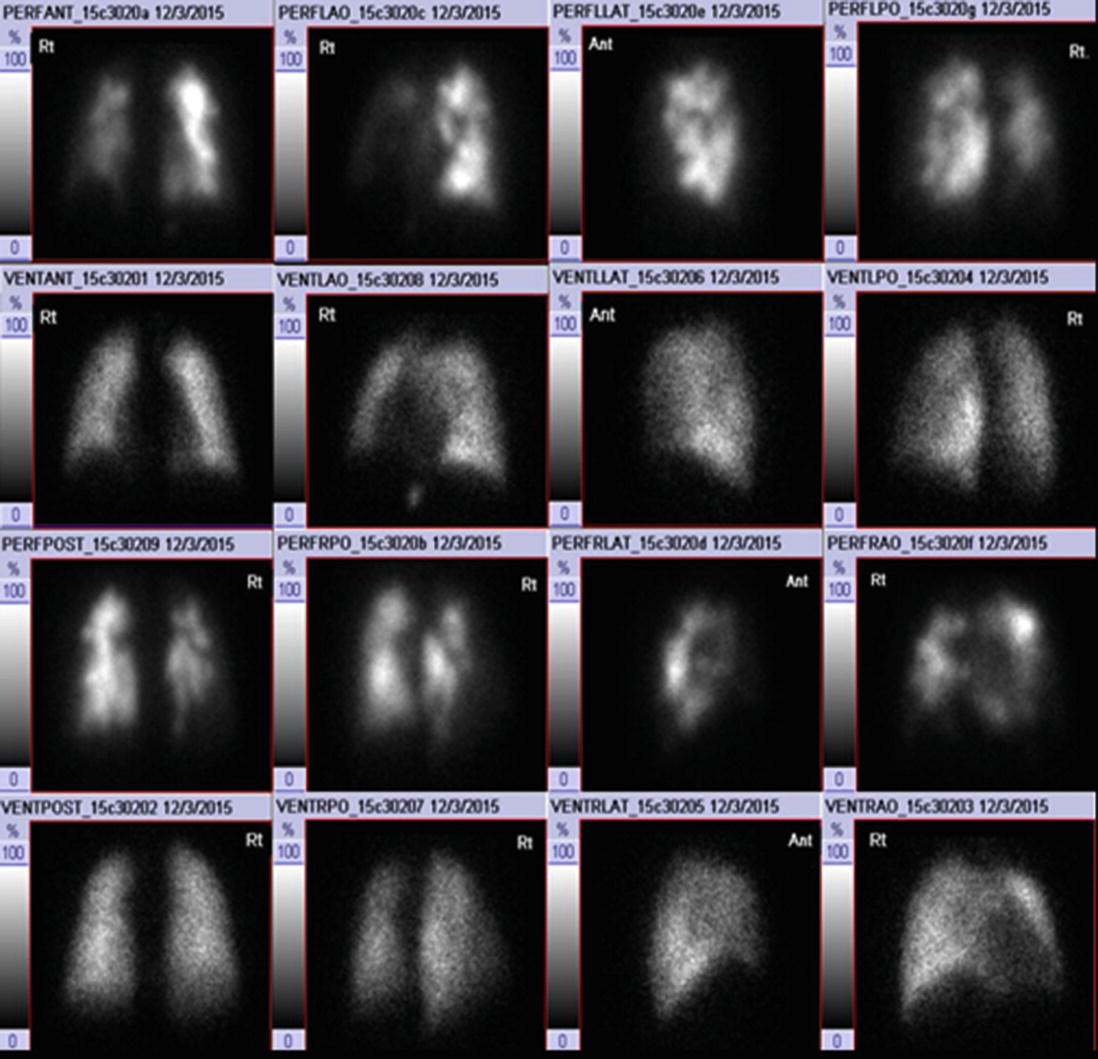
A ventilation perfusion (VQ) scan (Fig. 12.2) to screen for chronic thromboembolic disease revealed numerous segmental and subsegmental mismatched perfusion defects bilaterally with modestly decreased perfusion noted to the entire right lung relative to the left.
Figure 12.2
Lung scintigraphy shows R > L bilateral segmental and subsegmental unmatched defects
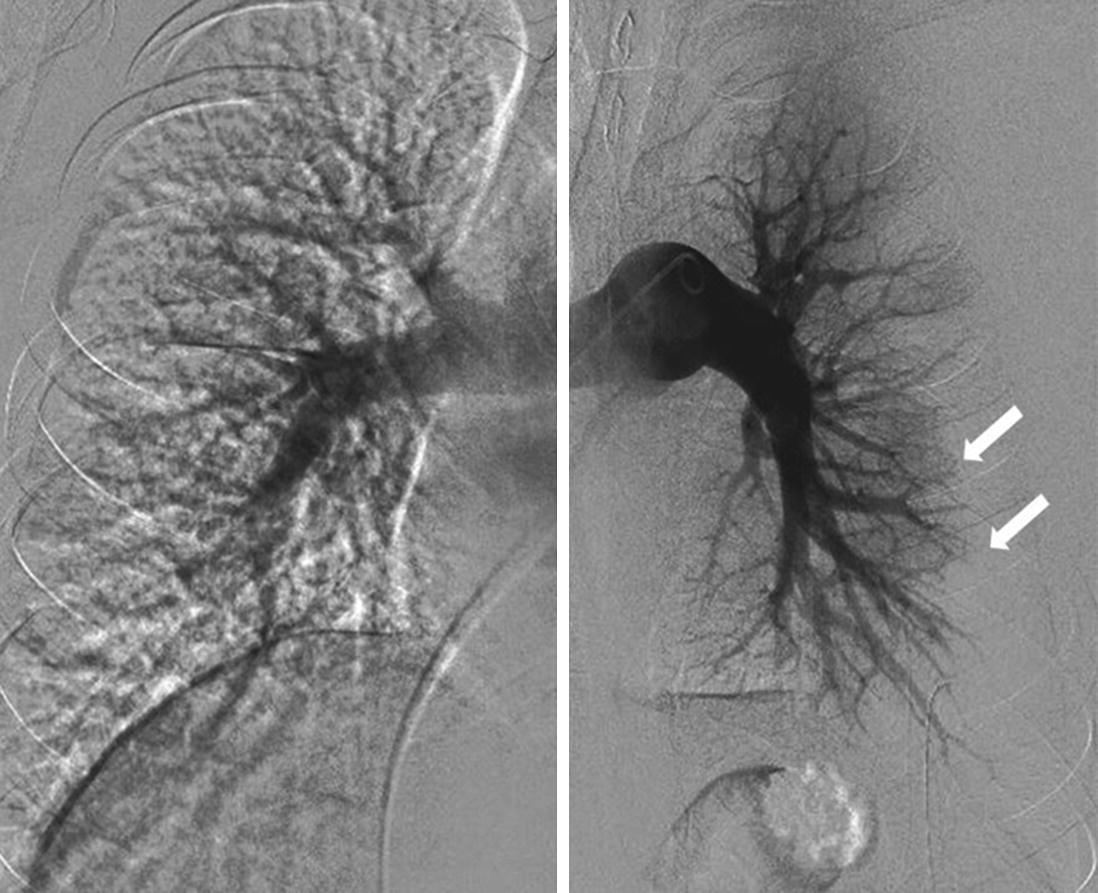
Right cardiac catheterization showed, in mmHg, right atrial pressure (RAP) 8/5/2, right ventricular pressure (RVP) 72/0/2, pulmonary artery pressure (PAP) 73/37/46, pulmonary capillary wedge pressure (PCWP) 5. Pulmonary arterial oxygen saturation was measured at 62% with a cardiac output and cardiac index obtained by Fick method of 6.42 L/min and 2.69 L/min/m2 respectively. Pulmonary angiogram was also performed showing multiple cut-off’s in the right upper, middle, and lower lobes that was interpreted to be due to a large burden of chronic thrombus in the entire right lung. Small cut-off also noted in the left upper anterior artery consistent with chronic thrombus (Fig. 12.3).
Figure 12.3
Pulmonary arteriogram shows a reduction in peripheral perfusion or “pruning” in the left lower lobe (arrows)
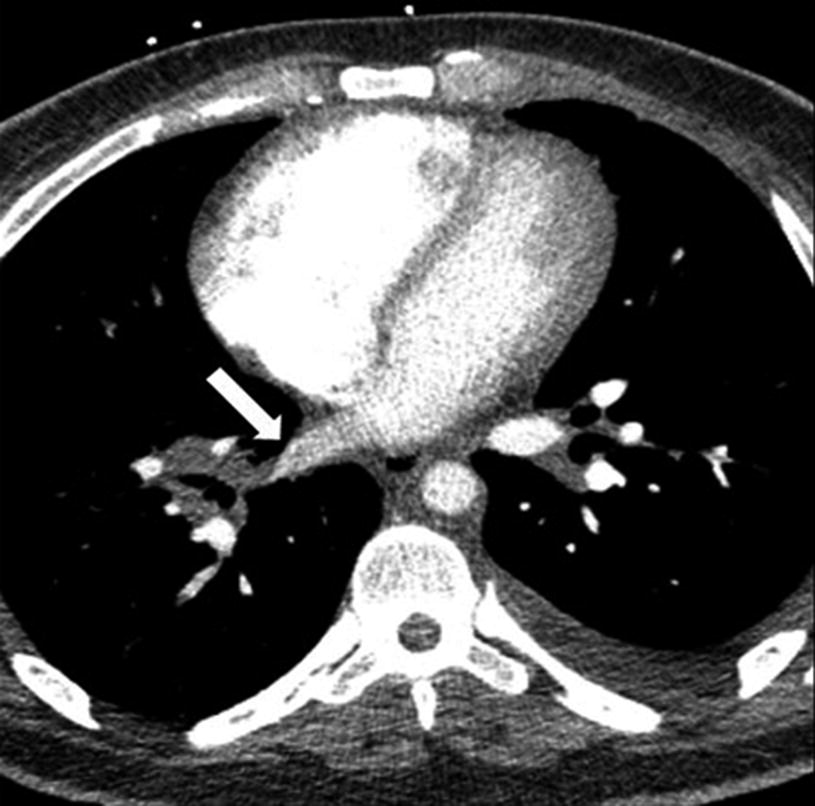
A multi-disciplinary meeting was held including the Pulmonary Hypertension Team, Interventional Cardiology who had performed angiography, the Chest Radiologist and CT Surgery. In light of the V/Q scan findings and the interpretation of the PA gram, despite the absence of evident thromboembolic disease by CTA, CTEPH was entertained as the probable diagnosis. There was further concern for the possibility of large pulmonary venous thrombosis on CTA (Fig. 12.4).
The patient was started on unfractionated heparin while inpatient and discharged home on long term anticoagulation for chronic thromboembolic disease. His diagnostic testing was sent to the University of California in San Diego for an assessment of operability.
Figure 12.4
CT angiogram of the chest show a flow disturbance in the right inferior pulmonary vein (block arrow)
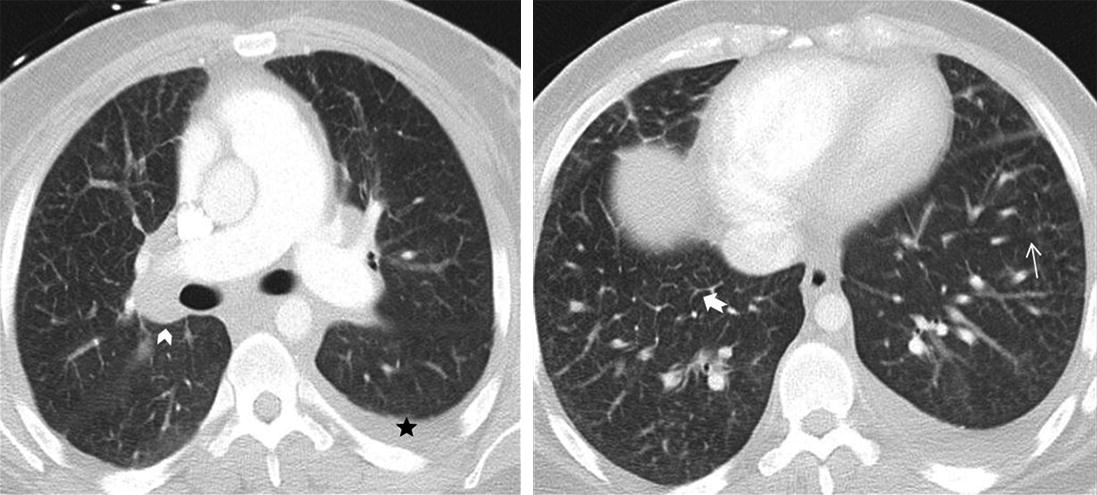
The patient presented to the hospital one month later with worsening dyspnea, now occurring at rest. Physical examination was significant for normal S1 and S2 with prominent P2, grade 2/6 holosystolic murmur heard best a left upper sternal border, JVD of 8 cmH2O, and 2+ lower extremity edema. There was significant progression of CT imaging findings (as below), with increase in interlobular septal thickening and areas of ground glass opacities with stable lymphadenopathy (Fig. 12.5).
Figure 12.5
CT angiogram shows bilateral diffuse ground glass opacities (thin arrow), smooth interlobular septal thickening (notched arrow), pronounced mediastinal and hilar lymphadenopathy (chevron) with a small left pleural effusion(black star)
Only gold members can continue reading. Log In or Register to continue