Chapter 12
Questions
- 221. The following are potential complications of aortic valve endocarditis:
- A. Aortic root abscess
- B. Supra-annular mitral regurgitation
- C. Aneurysm of mitral–aortic intervalvular fibrosa
- D. Aneurysm of anterior mitral leaflet
- E. All of the above
- 222. The following statements are true about patent foramen ovale except:
- A. Pick-up rate is higher with saline contrast compared to color Doppler imaging
- B. Transesophageal echocardiogram (TEE) is more sensitive than transthoracic echocardiogram
- C. Yield is higher with leg injection compared to arm injection for saline contrast
- D. Present in about 50% of normal population
- 223. Saline contrast echocardiography in a patient with cirrhosis of the liver showed appearance of contrast in the left atrium five beats after its appearance in the right atrium. This is suggestive of:
- A. Normal physiology
- B. Hepatopulmonary syndrome
- C. Patent foramen ovale
- D. Portopulmonary syndrome
- 224. Which type of aortic valve is least likely to be repairable for correction of severe aortic regurgitation?
- A. Failure of leaflet coaptation due to severely dilated ascending aorta with structurally normal leaflets
- B. Bicuspid aortic valve with prolapse of the conjoint cusp
- C. Aortic intramural hematoma with extension to the base of right coronary cusp causing it to prolapse
- D. Rheumatic aortic valve disease
- 225. TEE was performed intraoperatively following coronary artery bypass grafting (CABG) because of failure to wean from cardiopulmonary bypass. It showed akinetic inferior wall with 3+ mitral regurgitation originating at the medial commissure. These findings were not present preoperatively. The inferior wall looked excessively bright. Most likely problem in this patient is:
- A. Air embolism into right coronary artery (RCA)
- B. Thrombosis of RCA graft
- C. Excessively high blood pressure
- D. Excessive intravascular volume
- E. Poor myocardial preservation
- 226. The image is suggestive of:
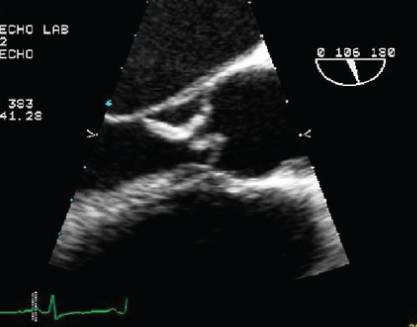
- A. Aortic dissection
- B. Aortic valve endocarditis
- C. Unicuspid aortic valve
- D. Hypertrophic cardiomyopathy
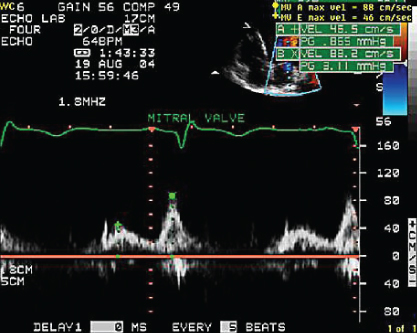
- 227. Continuous wave Doppler shown here could be a result of:
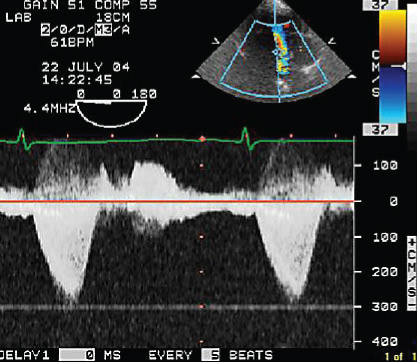
- A. Hypertrophic obstructive cardiomyopathy
- B. Severe mitral regurgitation
- C. Tricuspid regurgitation
- D. Ventricular septal defect
- B. Severe mitral regurgitation
- 228. In this figure, number “1” denotes:
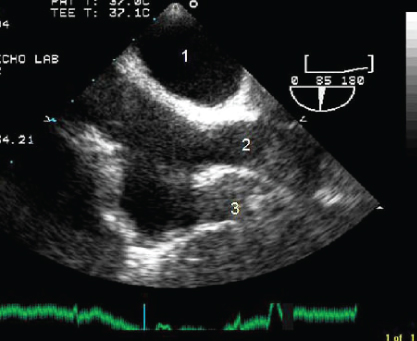
- A. Left atrium
- B. Right atrium
- C. Aorta
- D. Right pulmonary artery
- 229. In the figure, number “2” is:
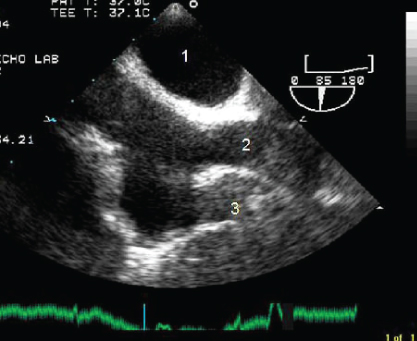
- A. Superior vena cava
- B. Inferior vena cava
- C. Pulmonary artery
- D. Aorta
- 230. In the figure, number “3” denotes:
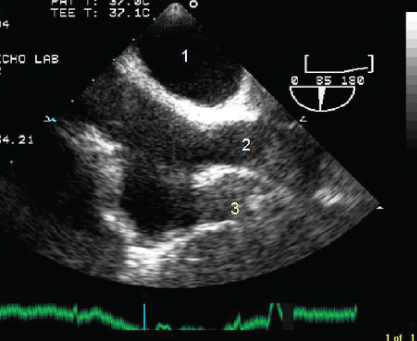
- A. Left atrium
- B. Right atrial appendage
- C. Inferior vena cava
- D. None of the above
- 231. This image shows:
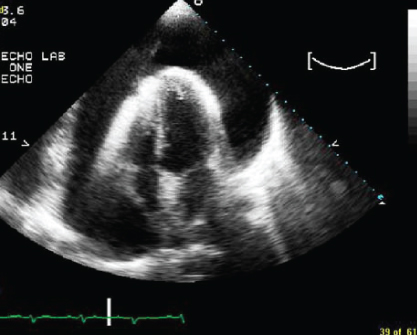
- A. Large left pleural effusion
- B. Large pericardial effusion with no evidence of tamponade
- C. Large pericardial effusion with features of tamponade
- D. Mirror image artifact
- 232. This mitral inflow pattern is consistent with:

Stay updated, free articles. Join our Telegram channel
- A. Aortic root abscess

Full access? Get Clinical Tree


