History
A 58-year-old male office worker with a long-standing history of cardiomyopathy, likely after an episode of viral myocarditis 20 years previously, sought treatment for worsening shortness of breath and functional deterioration. The patient was mildly obese and not in acute respiratory distress. He had a dual-chamber pacing system because of intermittent heart block and symptomatic sinus bradycardia while on medical therapy.
Because of ventricular dysfunction with a left ventricular ejection fraction (LVEF) of 28%, an implantable cardioverter-defibrillator (ICD) was recommended. The patient also had symptomatic heart failure (New York Heart Association [class III]) despite optimal medical therapy and a left bundle branch block with QRS duration of 148 ms. Cardiac resynchronization therapy (CRT) also was recommended.
He was taken to the procedure room at his local facility for upgrade to a CRT defibrillator (CRT-D) system. However, because of inability to place the left ventricular lead, the procedure was abandoned and the patient was referred for consideration of an epicardial system or to reattempt endocardial left ventricular lead and CRT-D placement. The operative note from the outside facility mentioned difficult subclavian venous access and inability to pass a wire beyond approximately 2 cm into the coronary sinus.
Past medical history is significant for intermittent atrial fibrillation, associated with mild symptoms and managed with rate control and anticoagulation.
Current Medications
The patient was taking lisinopril 10 mg twice daily, carvedilol 25 mg three times daily, and digoxin 0.125 mg once daily.
Physical Examination
Hospital and Procedural Course
After discussing the options of reattempting left ventricular lead placement, surgical epicardial lead placement, and assessment for appropriateness of left ventricular assist device or cardiac transplantation, it was decided to make another attempt at placing the coronary sinus lead before considering the other options. Another attempt at a transvenous approach was favored because of the benefits it offered over epicardial pacing, including lower surgical trauma, potentially more stable pacing electrical thresholds, and greater lead stability.6
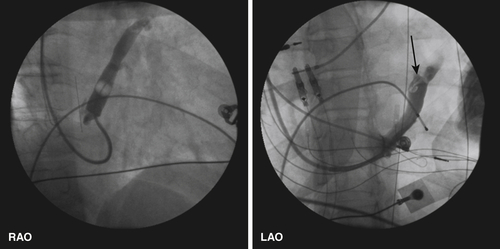
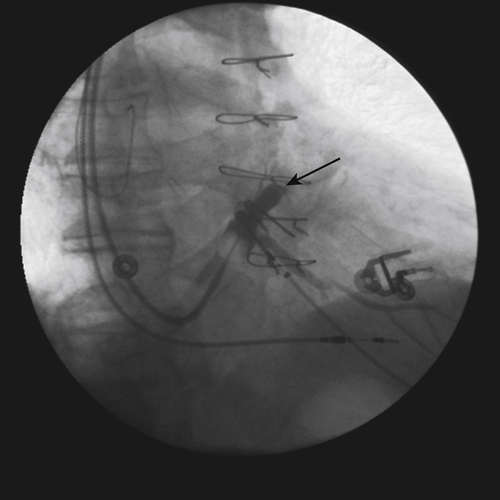
The patient was brought in the fasting state to the procedure room. An axillary vein puncture was done with contrast venography, and a temporary pacing lead was placed because the patient was pacemaker dependent. The coronary sinus was cannulated without difficulty and balloon venography performed.
Venography findings are shown in Figure 11-1. As noted in the operative report from the referring institution, a wire would not pass beyond approximately 2 cm into the coronary sinus.

Focused Clinical Questions and Discussion Points
Question
What is the likely cause of difficulty in advancing into the coronary venous system in this patient?
Discussion
Venography demonstrated a prominent Vieussens valve.2 The Vieussens valve is a normal anatomic variant and is an intravenous valve located at the junction of the coronary sinus and the great cardiac vein. This is typically the site of takeoff for the posterolateral ventricular vein and the oblique vein of the atrium (vein of Marshall). Studies have shown that a nearly occlusive Vieussens value, as found in this patient, can prevent progression of catheters and guide wires and complicate a cardiovascular interventional procedure.4 Therefore when various wires were passed into the coronary sinus, they would typically not advance beyond the valve and curve back into the main body of the coronary sinus.
Question
What are other potential reasons a wire will not pass freely into the branches of the coronary venous system?
Discussion
Once the coronary sinus has been cannulated, it may be extraordinarily difficult in certain patients to advance into the coronary venous system, particularly to the lateral free wall of the left ventricle. Potential reasons for this include coronary vein stenosis, intraprocedural coronary artery dissection, coronary vein dissection, and postsurgical or ablative therapy–related vein occlusion. In cases in which the target vein is obstructed and no alternative vessels exist, balloon dilation or stenting may be necessary for successful lead implantation. Although the frequency of coronary vein stenosis is reported to be about 2.4% in one study, balloon angioplasty proved to be an effective method when used in combination with careful maneuvering of guide wires and leads for nearly all the patients.5
Sharp angles at which veins enter the coronary sinus can further interfere with the successful advancement of guide wires and lead into distal regions of the coronary venous system.8



