PA and lateral chest radiograph showing cardiomegaly and enlarged central pulmonary arteries
Past medical history included hypertension, gastroesophageal reflux disease, depression, and a history of congenital atrial septal defect with repair at age 10 in 1975 followed by mitral valve repair with 28 mm Physio II annuloplasty ring as well as closure of A2 plus A3 and release of P3 chordae in 2010. A tricuspid valve annuloplasty and patch reconstruction of the right superior pulmonary vein were also performed at that time.
Social history was notable for no alcohol or illicit drug use but ongoing tobacco abuse with a 20 pack-year history.
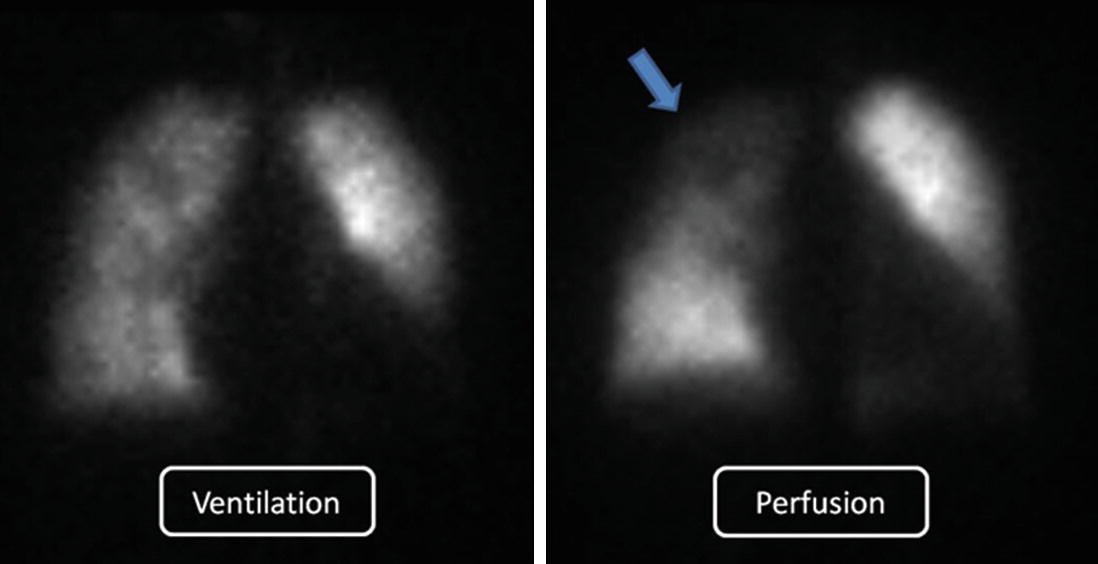
Hospital Course: The patient was diuresed with gradual improvement in dyspnea and oxygen requirement. Nonsteroidal anti-inflammatory therapy improved her musculoskeletal chest wall pain. An initial echocardiogram revealed severe pulmonic regurgitation with severe pulmonary hypertension with a pulmonary artery systolic pressure (PASP) estimate of 72, moderate right ventricular dysfunction and dilatation, with mild tricuspid regurgitation. Her left atrium was severely dilated and moderate diastolic relaxation impairment was noted. Mild mitral regurgitation was noted. No pericardial effusion was present. She was diuresed further and symptomatically improved with a repeat echocardiogram showing a PAPs estimate of 42. Bubble contrast administration revealed no evidence of shunting. Consultation with the pulmonary hypertension and cardiology service resulted in a differential diagnosis of WHO group 2 pulmonary venous hypertension, WHO group 4 chronic thromboembolic pulmonary hypertension (CTEPH), or chronic obstructive pulmonary disease (COPD) associated WHO group 3 pulmonary hypertension. Congenital heart disease associated pulmonary hypertension (PH) was deemed unlikely due to previous echocardiograms showing no PH as recently as 2010. Serologies for connective tissue disease, inherited or acquired hypercoagulability and human immunodeficiency virus were negative. Pulmonary function tests revealed a forced expiratory volume of 1.67 L (52% of predicted), forced vital capacity of 2.08 L (51% of predicted), a ratio between them of 80, total lung capacity of 3.66 L (52% of predicted), and a diffusion capacity adjusted for hemoglobin of 19.28 (72% of predicted) consistent with a moderate restrictive ventilatory defect with mildly impaired diffusion but no COPD. A ventilation-perfusion scan was performed (Fig. 11.2) and revealed unmatched perfusion defects to the entire right upper lobe (blue arrow).
Figure 11.2
Lung scintigraphy. Perfusion to right upper lobe is decreased (arrow) with intact ventilation
A computerized tomography pulmonary angiogram revealed no filling defects to suggest acute pulmonary emboli, with linear densities in the lower lobes and RUL suggestive of atelectasis.
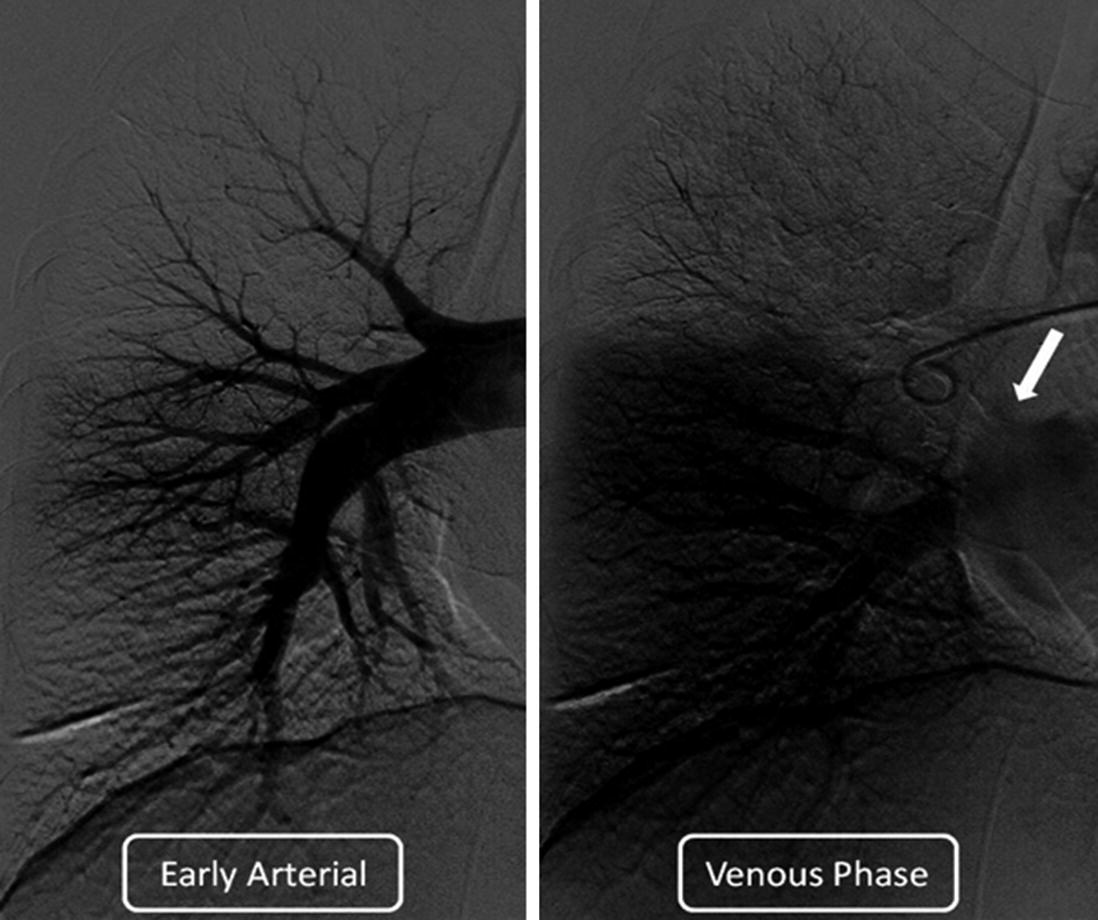
Concern over CTEPH prompted a combined right heart catheterization with pulmonary angiography. This revealed a right atrial pressure (RAP) of 10, pulmonary artery pressure (PAP) of 45/25 with a mean of 31, a pulmonary wedge pressure (PAWP) of 12, cardiac output (CO) of 4.61 L/min, cardiac index (CI) of 2.14 L/min, resulting in a pulmonary vascular resistance (PVR) of 4.12 Wood units. A saturation run revealed a high superior vena cava saturation of 66%, RA sat of 65.9 %, PA sat of 68.1%, with a systemic saturation of 95.5%. Inhaled nitric oxide at 40 ppm resulted in PAP of 50/23; mean of 32. A 500 cc rapid fluid bolus resulted in a doubling of the PAWP to 24. Pulmonary angiography (Fig. 11.3) revealed markedly decreased right upper lobe (RUL) perfusion with smooth stenosis of the truncus anterior.
Only gold members can continue reading. Log In or Register to continue